
The immunological mechanism of action for lost immunity, a shift to tolerance (and autoimmunity?) from the shots
Have we unleashed a plague of IgG4-related disease on a subpopulation of humans?

If you want some proof to show pro-COVID shot nay-sayers that these shots are detrimental to normal functioning immune responses, read them this. Before I get into this paper that should stop the presses and provide a one-way ticket for a lot of people to prison for the rest of their lives (as a best punishment), I refer to an earlier article that I wrote on immunological tolerance. I wrote this piece on July 10th, 2022, and now this group, who I may add have NO CONFLICTS OF INTEREST, have confirmed a mechanism of action of spike tolerance and so yes, the spike protein might be capable of destroying tolerance itself.

A paper was published in Science Immunology on December 22, 2022 entitled: “Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination”1 and it explains in wonderful detail how a class of antibody that commands a non-inflammatory response (more like tolerizing) is prominent in people who have been repeatedly injected with the modified mRNA COVID-19 injectable products.
Translation: Instead of the intended pool of spike-specific neutralizing IgG antibodies being dominant in multiply-injected people, a pool of antibodies associated with spike-specific tolerance are dominant in multiply-injected people.
Besides the tolerizing capacity, they also showed that the phagocytic enabling capacities were much reduced overall. These activities lead to clearance of viral pathogens. Reduce them → reduction in viral clearance capacity.
Importantly, this class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition.
They did not see this result in the case of the non-mRNA injectable product ChAdOx1 (adenoviral vector-based vaccine) or for tetanus toxoid and Respiratory Syncytial Virus (RSV). They checked. This confirms that this class switch to this tolerizing antibody subclass is specific to the effects of repeated injections with the Comirnaty products (we’ll have to check the Moderna mRNA-1273 products) and more importantly, that is not a typical consequence of repeat antigen exposure from either natural infections and vaccination.
To be clear, this wasn’t a ‘maybe the antibody profile was a little different’ type situation. This was a ‘whoa there’s a 48,075% increase in spike-specific antibodies between the 2nd and 3rd injections’ situation.
IgG4 antibodies among all spike-specific IgG antibodies rose on average from 0.04% shortly after the second vaccination to 19.27% late after the third vaccination.
Before I get into some of the details of what they did in this paper, some background is required.
Background on IgG1 and IgG4
Ig stands for immunoglobulin. These proteins are also called antibodies and there are 5 major types called IgA (the first line mucous guns: tears, saliva, mucous, blood-related), IgG (the plentiful guns: all body fluids related - especially blood/plasma), IgM (the big guns: blood and lymph-related), IgE (the allergic guns: lungs, skin, and mucous membrane-related) and IgD (the who-knows guns: gut-related?). The IgG antibody type has 4 subclasses: IgG1, IgG2, IgG3 and IgG4. I would like to focus to the first and last subclasses.
IgG1 is a subclass of antibody that responds to the presence of soluble proteins antigens and membrane proteins, so these are the guys normally associated with high levels in serum during and after viral infections. Deficiencies in this subclass can be associated with recurrent infections.2
IgG4 is a subclass of antibody that responds to repeated or long-term exposure to antigens, and ‘may become the dominant subclass’ as a result of this repeated exposure. Class switching to IgG4 may be modulated by Interleukin-10 (IL-10) and thus links this subclass of antibody to tolerance induction.3 It is really interesting that IgG4 may also represent the dominant antibody subclass in immune responses to the essential blood clotting proteins factor VIII and IX. Parasitic infections have also been found to be associated with the formation of IgG4 antibodies. (See reference #2).
*Regulation of IgG4 production is dependent on help by T-helper type 2 (Th2) cells and thus the IgG4 response is largely restricted to non-microbial antigens, like self-made spike proteins.4
Let’s get into some of the details of what they did. First, it is important to know that they looked at 2 independent test groups (N = 29 and N = 38) of healthcare workers who were injected 3 times with the Comirnaty product - the people who likely are exposed the most to all sorts of pathogens and thus, require the most robust defenses. They compared these two cohorts to another cohort of people who were injected with the adenoviral vector-based vaccine ChAdOx1 (AZD1222, Vaxzevria) and then got one shot of the Comirnaty product, and thus were able to distinguish between the specific antibody responses made between these cohorts and thus properly implicate the mRNA shots. Well, at least the Comirnaty shit. I mean shot.
In the following screenshot of Figure 1 B in the paper, they show data for 29 people who all had 3 doses of mRNA product. They measured the different IgG subclasses using flow cytometry and ‘recombinant monoclonal receptor binding domain (RBD)-antibodies as a standard’. For ease of eyes, they show the statistical comparison between the post 2nd data (10 days after 2nd dose), the follow-up (FU) post second (that included measurements after 210 days) and post 3rd (10 days after 3rd dose). The results speak for themselves.
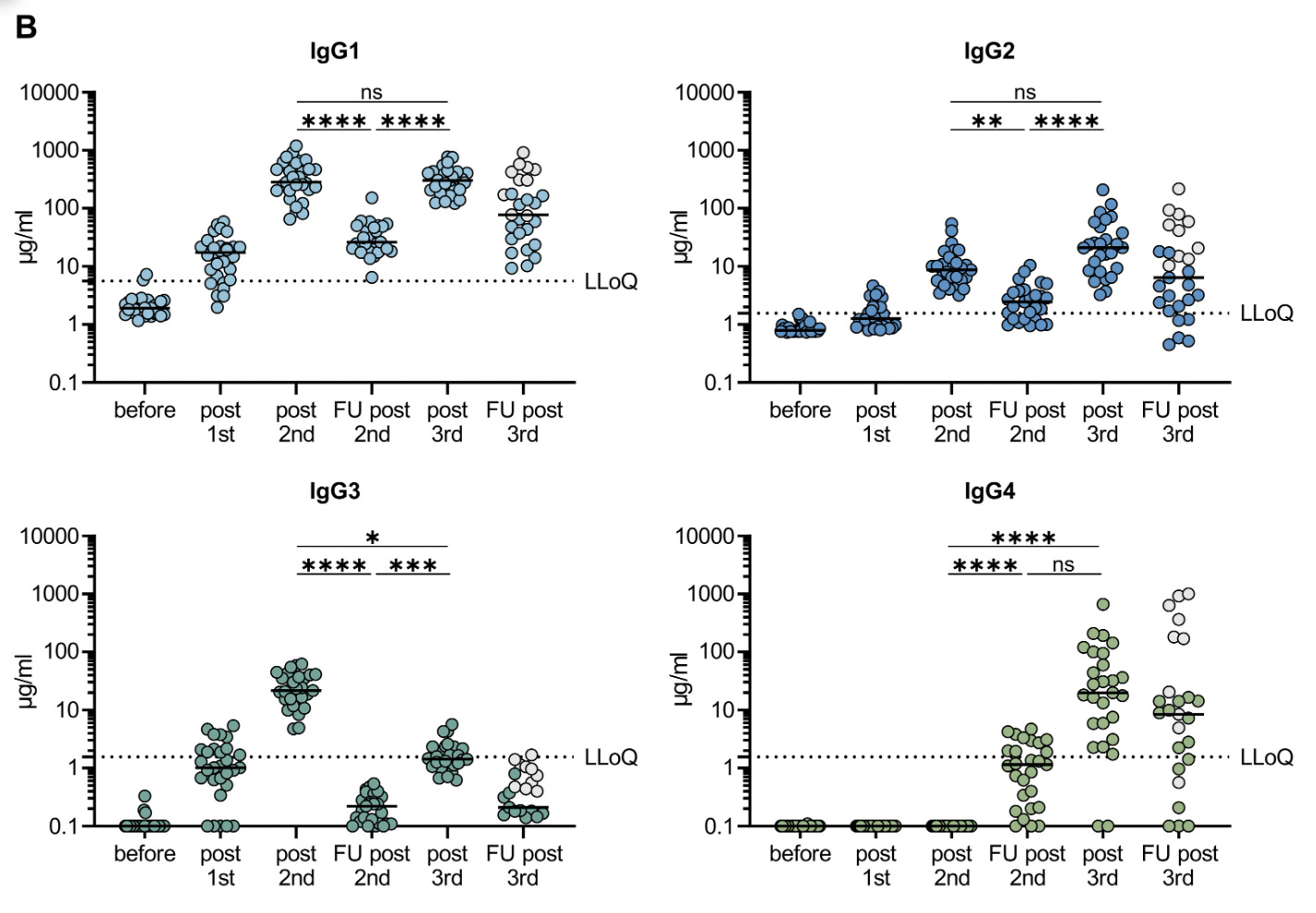
There are 4 plots in Figure 1 showing the antibody responses and measurements for IgG1, IgG2, IgG3 and IgG4 following injections with the Comirnaty products. I want to draw attention to the bottom right plot. This plot clearly shows the difference in the IgG4 antibody response in these people following the 3rd shot. Although IgG1 also attains high levels post 3rd dose (IgG1 is important for clearing viral pathogens), it concerning that the IgG4 level is so high due to its function as a tolerizing antibody, as opposed to a ‘clearance’ antibody.
In four individuals IgG4 even became the most prominent IgG subclass after the third immunization. Specifically in individuals having experienced an additional infection, IgG4 antibodies accounted for 40–80% of all anti-S antibodies.
Here’s a plot from Figure S1 in the Supplementary Figures that sums it up pretty good. This one also indicates the changing antibody subclass profile for people who experienced breakthrough infections.

They also characterized the spike-specific memory B cells according to their IgG subclasses using flow cytometry and the frequencies of IgG4 spike-specific memory B cells using scRNA-seq to check mirroring of serological IgG4 anti-spike levels. All confirmatory.
Another interesting finding pertains to the timing of the class switch to IgG4. It appears from their investigation that the switch is a consequence of ongoing germinal center maturation: it takes a few months for the IgG4-class-switched memory B cells to appear according to their results.
So the bottom line here is that the Cominaty product (again, we have to test the mRNA-1273 product) induces a shift away from a viral clearing to a tolerance-inducing antibody class, and this is not the status quo for traditional vaccines or natural infections. The main problem here is, once again, because this wasn’t checked (aka: NO LONG TERM OR EVEN SHORT TERM DATA), we have no idea of the effects of this ‘effect’.
It is at this point that I would like to introduce a disease related to IgG4 appropriately called IgG4-related disease. Original, right?
IgG4-related disease (IgG4-RD)5
So I had never head of this before today. This is a ‘dis-ease’ that is characterized by lymphocyte (white blood cell) and IgG4-secreting plasma (B) cell tissue infiltration.
The result of this infiltration is fibrosis (scarring).
Any tissue involved is subject to the formation of masses and tissue-destructive lesions - all with characteristic histopathological appearances.
This ‘dis-ease’ is relapsing and remitting, which means it comes and goes, and during the acute phase - the part where it ‘comes’ - “in approximately 51–70% of people with this disease, serum IgG4 concentrations are elevated”. (See reference #4). It has been well-documented that steroids can help with this ‘dis-ease’. This would also explain why steroids work well in people suffering from both COVID and adverse event reactions. Ahem.
Inflammation and the deposition of connective tissue in affected anatomical sites can lead to organ dysfunction, organ failure, or even death if not treated.
This sentence blew my mind.
Connective tissue diseases have been on my mind - and research plate (on the plate of Stephanie Seneff, as well) - for weeks now. I have been trying to figure out what those white stringy, gummy protein deposits are that are being found lining the blood vessels of the dead since 2021. It lead me to start researching connective tissue diseases.
I am researching this as we speak so will continue on this subject matter in my next Substack but before I go, one more thing.
Molecular mimicry has been shown in multiple publications to be a potential problem with regard to the spike protein whereby it has been shown to share motifs with human proteins. What this means is that autoimmunity potential against these human proteins is clear and present. In the context of this recent publication showing a dominant IgG4 pool, I have to wonder what the implications of this dominant pool are for molecular mimicry. Are these IgG4 antibodies capable of tolerizing in the context of our own proteins?
Please read the following for some background on this.
To be continued in an upcoming Substack…
I would be remiss if I did not give a shout out to Arkmedic
and Joel

and Brian here. :)

Irrgang P, Gerling J, Kocher K, Lapuente D, Steininger P, Habenicht K, Wytopil M, Beileke S, Schäfer S, Zhong J, Ssebyatika G, Krey T, Falcone V, Schülein C, Peter AS, Nganou-Makamdop K, Hengel H, Held J, Bogdan C, Überla K, Schober K, Winkler TH, Tenbusch M. Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci Immunol. 2022 Dec 22:eade2798. doi: 10.1126/sciimmunol.ade2798. Epub ahead of print. PMID: 36548397.
Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. 2014 Oct 20;5:520. doi: 10.3389/fimmu.2014.00520. PMID: 25368619; PMCID: PMC4202688.
Akdis CA, Akdis M. Mechanisms of immune tolerance to allergens: role of IL-10 and Tregs. J Clin Invest. 2014 Nov;124(11):4678-80. doi: 10.1172/JCI78891. Epub 2014 Nov 3. PMID: 25365074; PMCID: PMC4347251.
Aalberse RC, Stapel SO, Schuurman J, Rispens T. Immunoglobulin G4: an odd antibody. Clin Exp Allergy. 2009 Apr;39(4):469-77. doi: 10.1111/j.1365-2222.2009.03207.x. Epub 2009 Feb 13. PMID: 19222496.
https://en.wikipedia.org/wiki/IgG4-related_disease
I don't think I have ever seen such a dramatic and coordinated realisation of something that we all felt to be true as this over the last few days.
We have all had to say something
https://arkmedic.substack.com/p/philadelphia-2023
At first I thought only poor research and the push for $$$$. As investigators like you, Eugyppius, Ethical Skeptic, etc, etc, continue to point out the idiocy of policies and the ignored research it becomes more difficult to not think conspiratorially. As the research results get more frightening I get more confident that my wife and I (both 73 yr old) made the correct decision about these "vaccines." Thanks for continuing to push on all this. Once again the case is made for discontinuing these injections once again the signals are ignored.