


A possible aetiology for Dose 2 and Dose 3 responses seen in Myocarditis post COVID-19 injectable product administration?
mmm K. Probably not.

Dose 2 and Dose 3 effects observed in myocarditis reports in VAERS post-COVID injectable product administration are shown below in Figure 1 . The plots represent reports versus age and dose according to the Domestic (left) and Foreign (right) data sets.
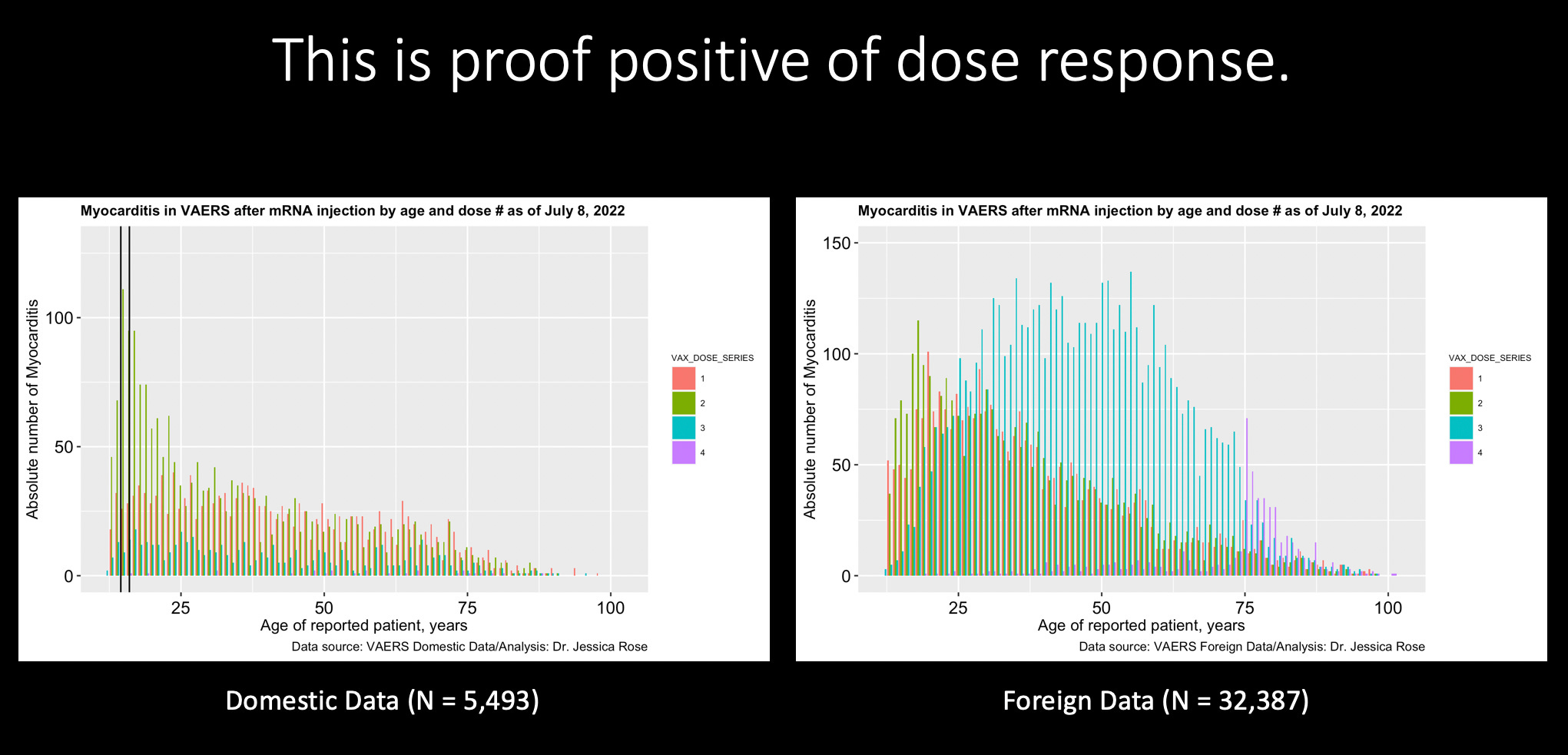
I wrote this Foreign data Dose 3 response effect up in a previous Substack article so please feel free to read that one.
These Dose 2 and 3 effects are more visible in the Pfizer data (left).

So let’s focus on Pfizer from here on out, shall we?
Just today, July 20, 2022, I posted another Substack article about a disclosed ingredient in the Pfizer injectable product ingredient list classified as ‘Hazardous’ called Potassium chloride (KCl). You should read that article first. You’ll be interested to know that Moderna does not, and never did have, KCl listed as an buffer component and when you go to the URL to check this information, you get a dead link.1
Question: What does this mean for the children who are diagnosed with myocarditis in temporal association with these shots?
By ‘this’, I meant repeatedly injecting children with a myocarditis diagnosis with a product that has a potentially damage-inducing concentration of KCl in it. KCl should only be used as a therapeutic in the context of hypokalemia or low serum levels of potassium.
According to the Pfizer Package leaflet: Information for the recipient COVID-19 mRNA Vaccine BNT162b2 concentrate for solution for injection tozinameran, they claim that there’s nothing at all in the way of potassium in their shots! Nothing at all! NOTHING at all! NOTHING AT ALL!
Here is a screenshot of the claimed concentration of potassium in a single dose.

An average child weighing 36 kg will have about 2.65 L of blood in their body.2 It was pointed out by a reader named Jim H that in my previous post, the KCl was < 1% by weight. True. So to be fair, the amount of KCl per IM dose is likely far less than 39 mg which may be, as Jim H pointed out, a technical threshold. It is likely to be a few mgs. The dose volume of the Pfizer product after dilution with 1.8 mL sterile 0.9% Sodium Chloride Injection is 0.3 mL. So this means that there is likely just a few mgs of potassium in that 0.3 mL dose.
Therefore, the exogenous serum concentration of potassium following a single dose injection for a 36 kg child would be very low. In a healthy child greater than 1 year of age, normal serum potassium levels are 3.5 to 5 mmol/L.3 Hyperkalaemia, which is excessive (or increases in) serum potassium levels (plasma-potassium concentration above 6.5 mmol/L or in the presence of ECG changes), in children is a very rare condition and is life-threatening.
True hyperkalaemia is a rare but life-threatening emergency. All children with true hyperkalaemia require immediate hospital assessment and management.4
So if a child was in the upper range of potassium serum levels, the exogenous increase from the shot would probably not make a difference. But, this is assuming that Pfizer is not lying about the concentration of potassium per dose.
I would also like to ask Pfizer why they added this component to the buffer in the first place if it’s ‘essentially potassium-free’! What was the point? And…
***This just in thanks to the mouse patrol! (Say that like JP Sears.) KCl was removed from the ‘new’ buffer formulation.5 Why would they do that? Too many exacerbated cardiac incidents in kids, eh? They likely removed KCl as a buffer component when they swapped out PBS for Tris in the kids’ magical unicorn formulation in October 2021.6 7
We were all wondering, why did you do that? But ours is not to question the raging psychotic profit monster and its goons who’s goal is to inject us all with their experimental products! How dare we! Oh Greta! How right you were! Barf.

I will return to the pre and post-inclusion of potassium chloride in a moment. Just as a teaser, I would expect that if there was a direct relationship between heart incidents involving arrhythmia/(myocarditis?) and potassium as a buffer additive in the Pfizer shots, then its removal should be associated with a reduction in reports of heart incidents/(myocarditis?). Pfizer is more heavily associated with myocarditis reports in VAERS. The ratio of reporting is 1.7:1 (Pfizer:Moderna) in VAERS currently (July 15, 2022).
How likely is it that the potassium in the shots could be causing increased potassium serum levels and subsequent associated cardiac problems in children?
Of the 4 listed potential aetiologies of hyperkalaemia in children, drugs containing a large amount of potassium come in at number 3.

Now ‘large’, again, doesn’t seem to apply here according to the above calculations but still, we’re assuming I did the calculations right and that Pfizer aren’t lying.
Unfortunately for us, “symptoms are nonspecific and include muscle weakness and fatigue. Severe hyperkalaemia may cause either palpitations or syncope secondary to cardiac conduction disturbance”.8
ECG and blood work to assess renal function are par for the course when this highly rare condition is suspected. Hyperkalemia in children will reveal the following abnormalities with regard to ECG.
By the way, if exogenous potassium is the aetiologic agent, then the way to cure the child is to stop administering the exogenous source of potassium. Which they did! Curious that.
My next stop are VAERS myocarditis reports with associated ECG abnormalities. I wanted to check how many myocarditis reports currently filed in VAERS are associated with the clinical markers of Hyperkalemia.

The highest frequency of reporting is for 25-39 year olds and the second highest is for 12-17 year olds.
Back to the point about potential differences in reporting of myocarditis in VAERS pre and post-removal of potassium chloride from the buffer. Some important points have to be made here:
We don’t know if potassium has anything relationship to myocarditis reports associated with abnormal ECG. It’s likely that it doesn’t based on the low quantity in the dose.
We don’t know exactly when they swapped the buffers out. I will assume that they did it ‘universally’ when they started injecting 5-11 year olds in the first week of November 2021. Certainly, the children ages 5-11 were not getting a dose of KCl after November 7th, 2021 in their Pfizer shots. Heavens, no!
VAERS has a huge backlog. It is unknown if the majority of reports of myocarditis for 2022 are even in the front-end system yet. Let’s assume that they are.
We don’t know if the adult formulation was swapped out at the same time as the kids, or when, as mentioned above. We could assume it happened in November, but remember that adults received/are receiving old lots and batches and either Pfizer or Comirnaty in Dose 1, 2, 3, …, n. What a shit show, eh? It’s possible that we can’t know how many individuals greater than 11 got the non-potassium shots.
It is unfortunate that the 5-11 year VAERS reports of myocarditis are likely still in the backlog.
Assumptions:
Survey reports of abnormal ECG-associated myocarditis reports in context of Pfizer manufacturer from VAERS (combined Domestic and Foreign counts)
Survey reports for children ages 5 and above with 2 doses
Survey reports for children ages 5 and above with 3 doses
Separate the reports pre and post-November 7th, 2021 as per the Received Date
Here’s what we get.

I gotta say, I am pretty surprised by this result. The data for the age group 5-11 is really limited so there’s no real meaningful conclusions to draw from it. It’s probably backlogged. I will be updating this when more data comes into the front end data set. I also want to acknowledge that this effect might be due to the PBS switch to TRIS and have nothing to do with the potassium.
I wasn’t expecting this.
I think I forgot to mention that the connection between the dose response and the potassium (in my mind) was the additive effect of the potential cardiac effects (messing with cardiac muscle) from the potassium. Lots of assumptions. Nothing is certain. Also, the fact that Hyperkalemia is primarily associated with arrhythmia and not myocarditis may mean this whole line of questioning and investigation was moot! I did learn a lot though.
https://www.ema.europa.eu/en/documents/product-information/covid-19-vaccine-moderna-epar-product-information_en.pdf
https://www.vinmec.com/vi/news/health-news/general-health-check/how-many-liters-of-blood-does-the-human-body-have/?link_type=related_posts
https://www.uptodate.com/contents/image?imageKey=PEDS%2F86501
https://patient.info/doctor/hyperkalaemia-in-children
Kis Z. Stability Modelling of mRNA Vaccine Quality Based on Temperature Monitoring throughout the Distribution Chain. Pharmaceutics. 2022;14(2):430. Published 2022 Feb 17. doi:10.3390/pharmaceutics14020430.
https://www.fda.gov/media/153447/download
https://www.fda.gov/media/153409/download
Dr Colin Tidy, Reviewed by Dr Anjum Gandhi. Hyperkalaemia in Children. Last edited 25 Jan 2017.
"Oh and I got a job offer to be a VAERS analyst for the CDC today."
OMG, you should contact the CDC directly, dump all your VAERS findings on them, and thank them for asking 😆 Then wait a bit and submit a FOIA request so you have evidence that they know what you know.
Great sleuthing Jessica! When this is all over, pfizer is gonna say “and I might have gotten away with it too if it weren’t for you meddling kids!” The bad guys masks ALWAYS get pulled off in the end.