


For the dermatologists: it ain't just about warts and allergic dermatitis no more...
There are currently (as of Jan 7, 2022) 156,769 people in VAERS with reports of skin problems post COVID-19 injection.

I had a request from a dermatologist to do skin problems in VAERS so here you go. I had forgotten about this string! Skin problems are one of the most prolifically-reported adverse event types. ‘Rash’ for example, is reported in almost 1/4 of people who filed reports to VAERS. It is #1 across age groups as well. Herpes is up there as well. Although herpes isn’t necessarily a skin condition, but we all know, it does manifest as skin eruptions/blisters, so I am counting it.
Here we go with age stratified reports (not normalized) according to CDC age stratification and by decade. 128 reports for 0-5 year olds? Again, what?

And by decade… uni-modal… normal. 517 reports from 0-10 year olds.

This is what the data looks like normalized to the CDC age stratification. The denominator for the 0-5ers is small - that’s why the normalized number is relatively large.

And check out how many immediate reports were made. Probably “Injection site erythema”. Probably.
But you know what’s absolutely marvelous here? That bump on day 7. That sounds immunological to me. I will pass this onto Dr. Chetty to see what he thinks. The only other category I have seen this bump one week post injection is in the actual immunological AE group. The second largest cluster of reports of skin problems are being made 7 days post injection. Hmm.

I plotted the top 17 reported skin problems according to type for only the reports made on Day 7 to try to find out if they are ‘immunologically-related’.

Sure enough, from top to bottom, redness, hives, rash, rash, itching, ‘reaction’, rash, itching, pain, hardening, redness, herpes herpes bo berpes, itching, inflammation, burning, blister (Pemphigus Vulgaris?). All of these are associated with immune system mediators/inflammation and various cell types. What could be so irritating to the skin in so many people? Is it that the irritation arises due to bad injection techniques? I would think so. The last blood draw I got was done by an completely incompetent person - I could have done it better myself and I am not officially trained in phlebotomy1. Seriously. Maybe hire some actual vampires.
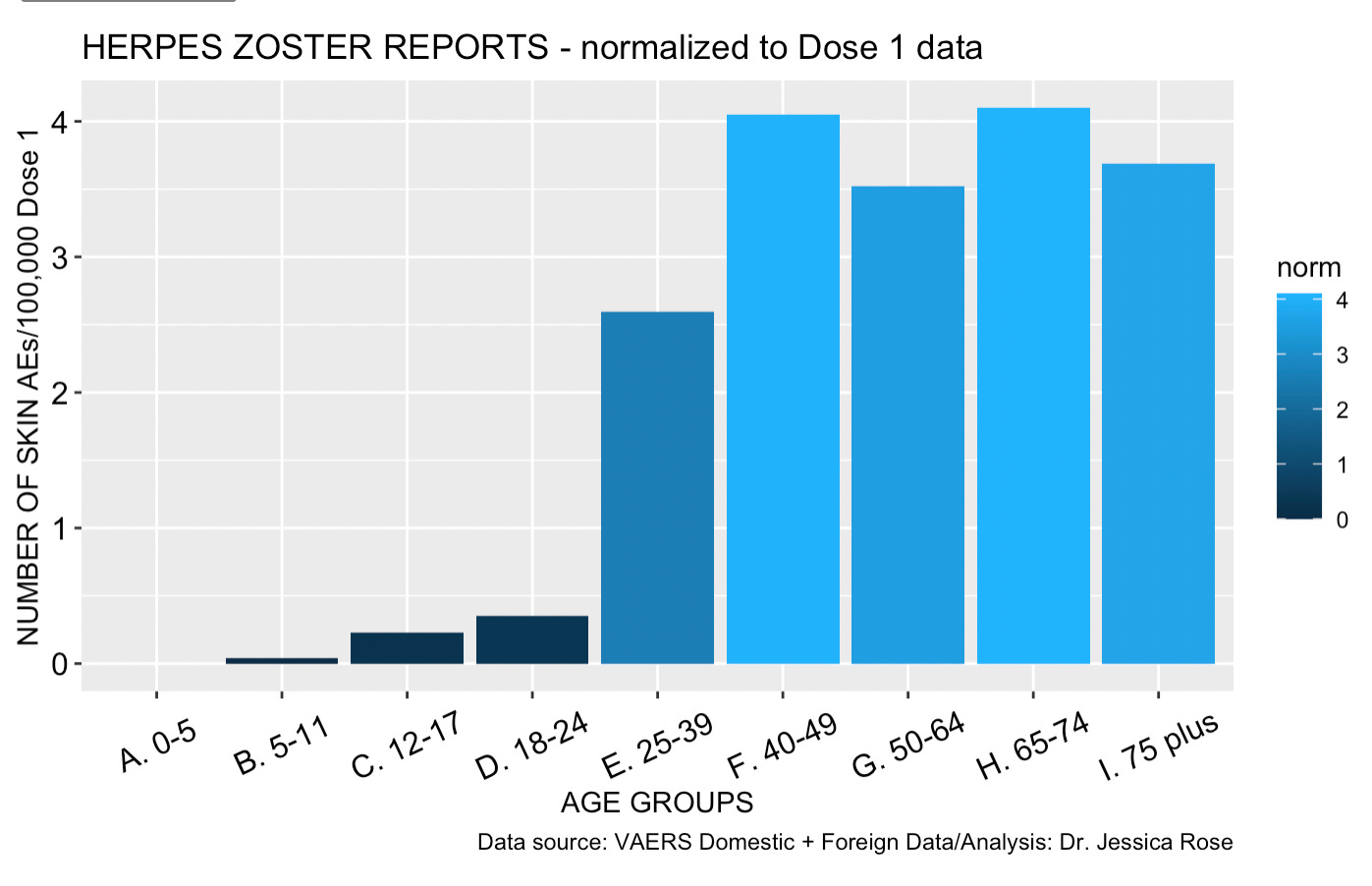
One more thing about Herpes zoster - which again, diagnostically is viral, yes, but it re-emerges due to immunological ‘off-guard-ness’ and manifests as weeping sores on the skin.
There are 9,992 reports of Herpes zoster. So far. Looks like this age-wise.

Normalized to dose 1 data looks like this. If you’re under 25, looks like you’re not reporting Herpes zoster outbreaks. Ideas?
I find all of this utterly fascinating but I must return to another project that is pending. Thank you again for getting to the end!
WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy. Geneva: World Health Organization; 2010. 2, Best practices in phlebotomy.
Jessica, it may be interesting to ask your VAERS skin problems requesting dermatologist if he is seeing more patients. If there is a reduction in immunity for those with the jabs, later skin issues may now be happening. A dermatologist client spike could be interesting to analyze.
Dermatologist here with a couple of observations:
1/ The vaccine-related dermatoses that we are seeing fall into the same pathologic categories being picked up by other physicians: Vascular injury eg. small vessel vasculitis, micro-thrombotic-related problems and immune-mediated issues which would include, for example, reactivation of latent viruses like HSV / VZV. 2/ I think all of these AEs are way underreported by dermatologists as we treat these conditions normally, and it is very difficult to definitively connect any one case to vaccination. And while I can't speak for other dermatologists, I have never reported anything to VAERS and would not take the time to do so unless the case were clear cut and resulted in some permanent damage. After all there is a big difference between "covid toes" or self-resolving superficial skin eruption versus covid injury to the myocardium or the production of some permanent neurologic deficit such as blindness or paralysis. It has been reported that the S2 portion of the spike protein may block tumor suppression via the P53 pathway https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7324311/ which plays an important role in some common skin cancers. It will be interesting to see whether mass vaccination has an effect on the incidence of skin cancer (and other cancers) in the future. But here also, it may be difficult to tease that signal out of the data.
What I find interesting is that the same mechanisms of injury appear to be involved across the board and kind of validate the pathophysiology involved with these injuries. Also, not to be snarky, but dermatology has always been about more than warts and allergic dermatitis.