


A short compendium of evidence to date...
Excerpt slides from various presentations of late...

I have become interested lately in more than just reporting on adverse event data and what’s going on in the peer-reviewed literature. I seem to be approaching a larger loop in the life spiral where I feel it’s time to summarize. So I attempted to do so in a meeting of doctors and lawyers last night. Here are some of the slides I presented. Feel free to add ideas and information so that we can make this slide deck even better. This IS the new peer review, after all! And if your ‘leaders’ won’t listen to you or take your ideas to heart, I WILL.
I always like to start with a bit a humor - albeit dark. Seems appropriate.

The modified spike protein: it was modified in many specific ways. Apart from the double proline mutation/substitution to maintain the pre-fusion conformation, uridines (U) were swapped out for pseudouridines (Ψ). Also, the entire mRNA was codon-optimized for use in humans. This basically just means that it was engineered to be as efficiently translated and expressed as possible in humans. Codon usage is organism-specific. This process necessarily introduces a higher GC (guanine and cytosine) content. The U to Ψ modification can lead to something called ribosomal pausing - a process that is inextricably linked to proper protein folding. Ribosomes are the protein machines that are fed the mRNA to allow transfer RNAs (tRNAs) to bring their amino acids over for translation and protein synthesis to ensue. This pausing at the exit door of the ribosome results in the ability of the protein to fold at specific sites such that the protein is folded correctly. ‘Improper’ ribosomal pausing can lead to protein mis-folding. This has to do with electrostatic forces as well, but I won’t go there now.
Protein function depends on the correct folding of the polypeptide chain into a three‐dimensional structure, with the exception of disordered proteins. Folding of such structured proteins often occurs co-translationally, i.e., at the ribosome, as the continuously elongating nascent chain emerges from the ribosomal exit tunnel.123
Think of a translator reading text in a language that it is familiar with. Then think of them coming across a dialect of this language - they might have to pause to figure out the meanings of some words. This can cause a ‘slow down’ in the translation process. And in biology, this can lead to amino acid chains getting ‘backed up’ and subsequent mis-folding. At least, that’s how I ‘see’ it.
The U to Ψ can also lead to ribosomal frame shifting that can lead to unintended proteins being produced and subsequent potential for additional, unintended mis-folded proteins. Codons are always in sets of 3 nucleotide bases so imagine one of the 3 doesn’t get read, for example. The reading frame of the mRNA might ‘shift’ to the next letter in the chain and subsequently, a third member of codon might become the first in a ‘new’ codon. This is still something I am learning about so feel free to add to this in the comments.
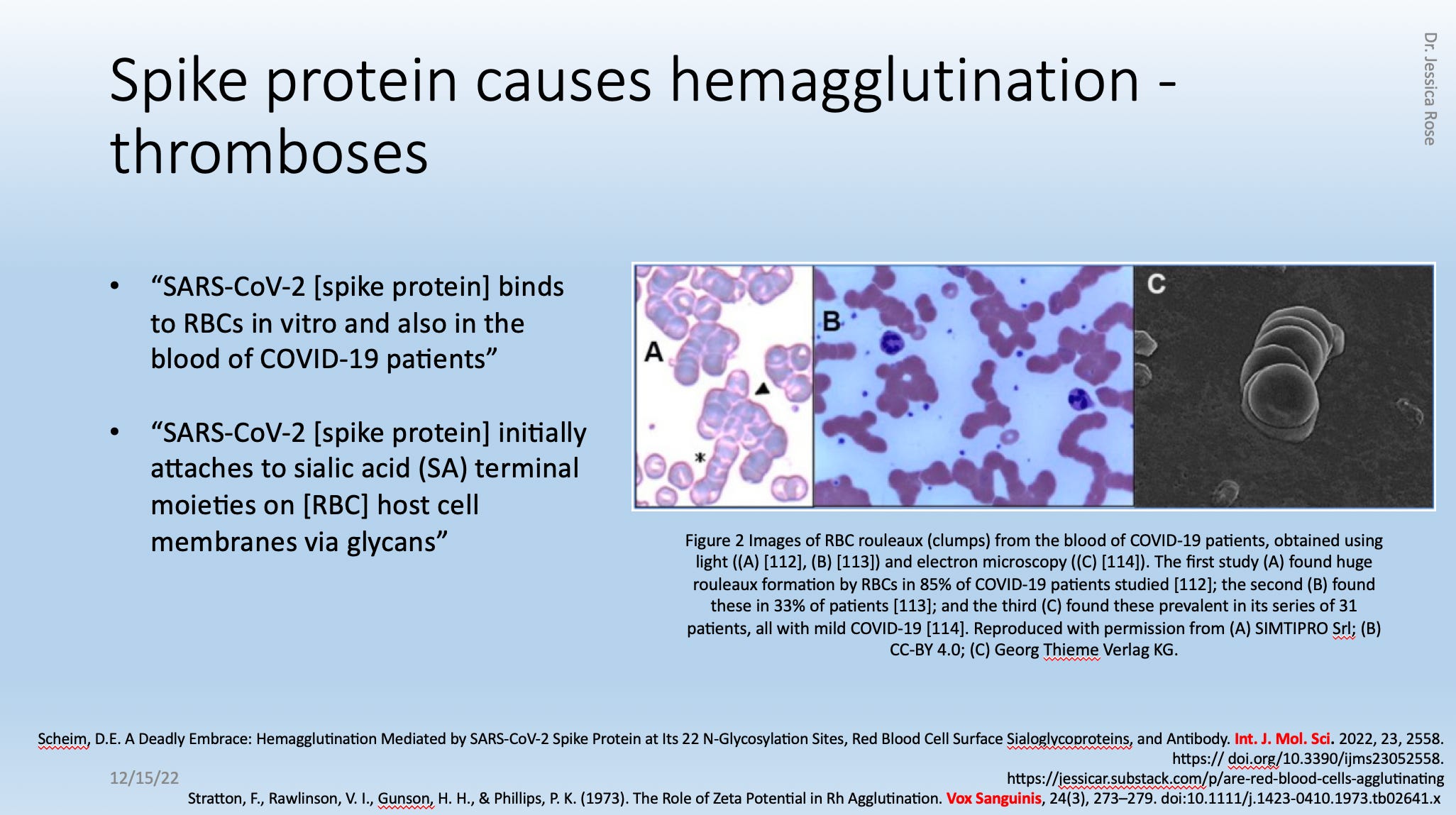
The above-referenced paper came out in February of this year (2022) and it shows an ACE-2/CD147-independent mechanism by which the spike protein acts like velcro to sialic acid-tipped glycans on red blood cells. Sounds like an ingredient for clumping and thrombotic events doesn’t it?

Many papers are being published that lend to the evidence pool that the spike protein contains peptides or ‘motifs’ that are identical to motifs in human proteins. What this means is that antibodies generated against the spike protein epitopes can also act against the human epitopes as autoantibodies, and cause potential pandemonium. Notice the long list of proteins with shared spike motifs and notice the associated tissues, organs or cells.

The next few slides are tidbits about %RNA integrity based on the above slide. There were some leaked documents that revealed that the COVID-19 injectable product batches that were tested in the lab had different %RNA integrity (on average) than the batches that were tested for use in people. The latter average was lower than the required Acceptance Criteria according to the European Medical Association, so they simply lowered the Acceptance Criteria to fit what they found to make it ‘Acceptable’ for use in humans, and to call these products into the ‘efficacious sphere’.

Now, even Pfizer admits that we need those mRNAs to be of a certain integrity in order for the product to be efficacious. Notice they refer to their product as a ‘drug’ - I do not disagree that these products classify far more suitably as pharmaceuticals (drugs) than biologicals. But, that comes with a whole other boatload of issues and I won’t go into that here. So was the %RNA integrity high enough to ensure ‘the efficacy of the drug product’, in reality? Who knows.

And what of the potential for ‘unwanted’ effects of having truncated RNAs being translated into smaller peptides and not full-length spike protein? Is this a better deal-io or a worse deal-io?

I counted the number of immunologically-associated reports in VAERS and to date, there are just under half a million. No under reporting factor considered here, by the way. These numbers far and away exceed anything reported for the past 30 years for all vaccines combined. The chart below shows only the VAERS absolute counts for Domestic data for the past 10 years by file size (left) and by number of VAERS IDs (right). See the difference? The CDC doesn’t.

It is also of interest on the subject of VAERS reports that a large percentage of people are still suffering.

No transience here folks. And I might add that in addition to the 42% of people reporting unresolved adverse events, 26% were reported as ‘unknown’ with regard to resolution, so it is entirely possible that the total percentage of unresolved reports in VAERS in 68%.

I also re-examined a question I had asked myself ages ago about the potential inverse relationship between expired products and severe adverse event (SAE) occurrence. It is interesting that over 100,000 people have reported being injected with expired products. No under reporting factor. Of these reports, a relatively low percentage qualify as severe.


It appears as though most people (79%) did not have an associated severe adverse event of those who were reported as having been injected with an expired product. Does this lend credence to the idea that people are better off with expired products because they have become inert?

It is exceedingly important that people know that the average percentage of SAEs for any year total, according to the VAERS handbook, is 15%. We have exceeded this average throughout the entire COVID-19 injectable product roll-out (since January 2021), with a peak in February 2021 of over 50%. We are currently at 24%, and this is exceedingly high.
ONE QUARTER OF ALL REPORTS FILED TO VAERS IN THE CONTEXT OF THE COVID SHOTS ARE CONSIDERED SEVERE? What? Anybody listening?

One last thing worth noting in the context of ‘efficacy’. Safe and EFFECTIVE, right? 76% of all people with reports in VAERS currently have associated COVID-19. Can you believe that? COVID-19 has been the #1 reported adverse event in VAERS for months, but it surprised even me when I did a search for COVID-19 in all the VAERS IDs by SYMPTOM, to find that 76% of these people have a COVID-19-associated MedDRA code included in their report.
The ironic injection? I think so. No, it’s not effective and it very clearly leads to productive infection - not reduction of transmission - enhanced likelihood of transmission, in fact. More sick people, more transmission. Way to go pharma, you got more patients. Harms? Exceeding amounts. Again, way to go.
So this is where we are. I leave you with my summary slide. We are in a place of choice, my friends. We either choose to end this. Or we do not.

Here’s some Radiohead excellence to perk up the day. I know this bass line inside and out.
Fedorov, A. N. & Baldwin, T. O. Cotranslational protein folding. J. Biol. Chem. 272, 32715–32718 (1997).
Kramer, G., Ramachandiran, V. & Hardesty, B. Cotranslational folding—omnia mea mecum porto? Int. J. Biochem. Cell Biol. 33, 541–553 (2001).
Wruck, F., Tian, P., Kudva, R. et al. The ribosome modulates folding inside the ribosomal exit tunnel. Commun Biol 4, 523 (2021). https://doi.org/10.1038/s42003-021-02055-8.
I find myself increasingly drawn to the issue of mRNA integrity and, specifically, the temperature requirements for the supply chain. This is an aspect which I don't think has been adequately looked at.
Even in the US and Europe the ability to transport, store and deliver products at -70 degrees is patchy at best. In ROW, non-existent. As a side issue, even if stored correctly through to the point of delivery, were there adequate storage facilities at the point of delivery and were adequate instructions available as to how the product should be taken from -70 degrees down to injection temperateure and how long the vials can be kept under normal refrigeration? I suspect there are a LOT of grey areas here!
Setting aside for a moment the issue of efficacy, perhaps the good news is that degraded RNA cannot do the same harm. At the extreme,, the issue here becomes perhaps the batches that have been reported to cause many of the AEs were NOT, in fact, the "bad" batches, but actually the "good" batches which had been correctly temperature-controlled throughout!!
It stands to reason that degraded product is less dangerous, especially for acute, serious reactions, the kind that will send a signal to VAERS. What's left is the pseudo-u and NLP's, and these may certainly be immunosuppressive, but you aren't going to get spike-related syndromes without much spike.
There are way too many people walking around who not only have been fine, but everyone they know is, as well. This sometimes applies even to people who are aware of the dangers, but are bewildered that it hasn't landed in their circle of familiarity. This can really only be explained by a systemic effect at the local level; i.e., lax protocols for handling and storage, or a deliberate shipment of inactive product.
What would you do, if you had a runaway train of adverse reactions and no longer cared as much about efficacy as keeping the warp core from melting down? A change in protocols would be the quick fix.