
The Tam emails...
Thank you to Bret Sears for the ATIPs

A thick of emails are heading our way as the product of Access to Information Act requests made by Bret Sears to have a look-see into Theresa Tam’s thinking (or lack thereof) since the onset of the COVID-era.
You can download and sift here.
I went through the first 2 of many docs. The first one is 265 pages and the other is 182. I saw a lot of stuff about “vaping”, some stuff on marijuana, DEI crap and a tidbit on fighting “vaccine hesitancy”.
The first document:
The "Addressing Vaccine Hesitancy in Ontario" proposal (pages 15-16) outlines a multi-pronged communication strategy to combat misinformation via school newsletters, websites, and printables. This reflects government interest in controlling narratives to ensure public compliance with health measures—like vaccination—crucial during “pandemics”.

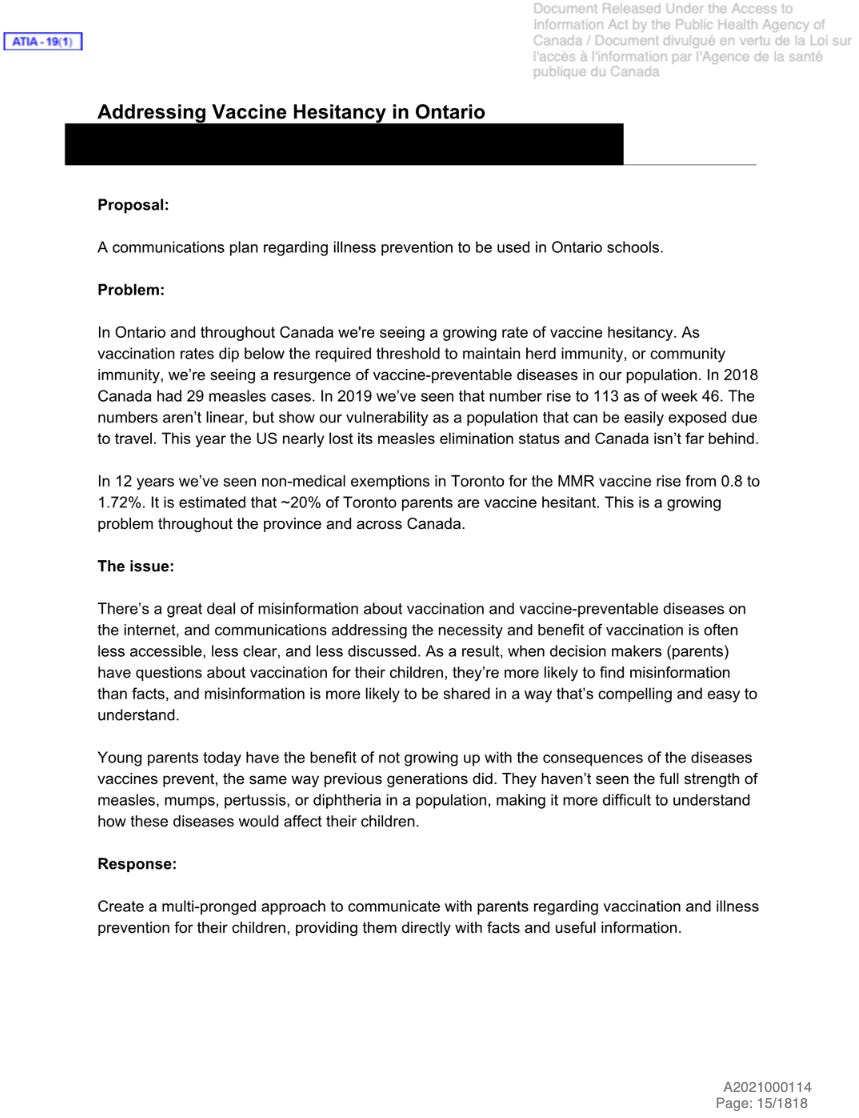
Isn’t that December 10, 2019 date… interesting?
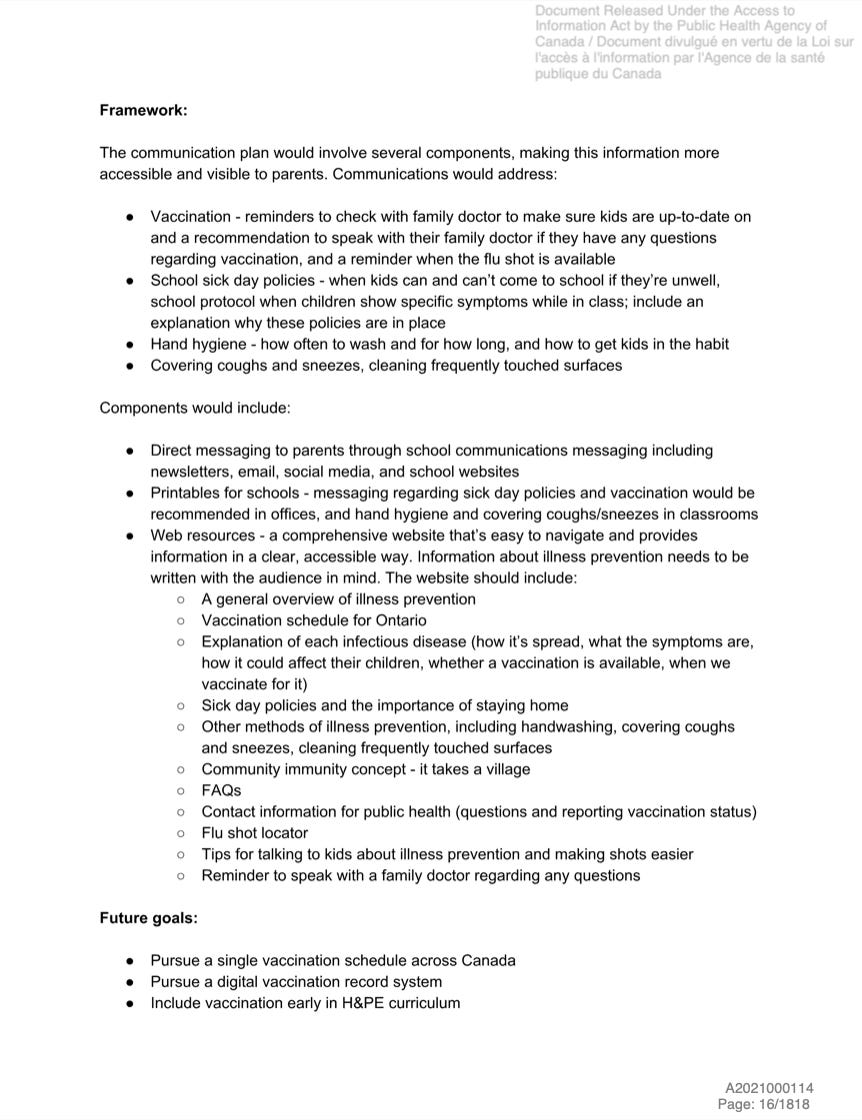
The “vaccine hesitancy proposal” suggests a standardized website with vaccination schedules, disease explanations, and FAQs, managed by public health authorities. This centralized approach could extend to “pandemic” messaging, consolidating government influence over public behavior. The proposal’s focus on integrating sick day policies and hygiene education into Ontario schools (page 16) shows how governments might use educational systems as control points for health enforcement, a tactic scalable to pandemics (e.g., school closures or vaccine mandates). Future goals in the proposal included a "digital vaccination record system" and a unified Canadian vaccination schedule.
These items suggest plans for government-controlled data systems, potentially for tracking compliance or managing pandemic responses.
Dr. Tam’s involvement in Adaptation 2020 (page 12), with a session on infectious diseases, indicates PHAC’s pre-COVID emphasis on climate-related health risks. This foreshadows government planning for broader health threats, including pandemics, though not yet specific to COVID-19. Roooiiigghhtttttt.

The second document:
The document highlights immigrant seniors’ isolation due to language barriers and limited service access. It is interesting that in the context of a “pandemic”, governments could prioritize these groups for targeted outreach, suggesting a control mechanism to ensure equitable health interventions.
Here are the highlights I found overall:

The above email is about development of a flu vaccine which you should know by now is a useless endeavor immunologically. Think of how and where that 1M$ could have gone to instead.

The email above discusses preliminary and disappointing results from the Nunavik Palivizumab program for preventing RSV hospitalizations in healthy full-term infants under 3 months. It’s disgusting how these poor people seemed to have no idea that they were part of an experiment.
Only ~60% of required Palivizumab doses were received, despite efforts.
Informed consent was lacking (big surprise there)
“Some ethical concerns were raised by health care workers regarding the guarantee of a free and informed consent from parents or caregivers, as well as the absence of involvement of Inuit population in the decision and implementation process.” This doesn’t sound like they care so much about RSV in the Inuit as much as they want to experiment on them with their pointless injections.
No prior data existed on Palivizumab’s effectiveness in healthy full-term babies, and results show it failed to prevent RSV hospitalizations effectively.
Many Nunavik babies hospitalized with RSV were co-infected with other viruses, potentially affecting outcomes.
Low cost-effectiveness (~$200,000 CAD per hospitalization prevented), and administrative issues may have impacted the program.
This is important to know about because of the onslaught of gene-based RSV therapeutics on the way. Again, a pointless endeavor immunologically.
The following shows involvement with the WHO in terms of funding. I wonder what they meant by “upcoming strategic dialogue” and “governance”?


More to come…
"Low cost-effectiveness (~$200,000 CAD per hospitalization prevented), and administrative issues may have impacted the program."
"...assumed effectiveness of Palivizumab at 30%..."
Is that newspeak for modelled assumption which failed?
At $200K a baby..
So for every 10 babies they achieve "assumed effectiveness" for 3.
Which means 10 babies times $200K is $2 Million
For an "assumed effectiveness" for 3.
Wow..nothing to see here folks..
Seems to be a very "1984" style of approach to heath care decisions. It would be nice to know if these interventions were actually safe and beneficial. I'm now 82, (COVID) unvaccinated and have never been sick with even a cold since the onset of the "pandemic." As far as I know I'm not included in any statistics.