


Increased susceptibility to SARS-2 infection/COVID-19 - signal emanating from VAERS in reports of breakthrough infection
A manuscript and hopefully a new paper in the making...

Abstract
Background: Millions of individuals have reported adverse events (AEs) using the Vaccine Adverse Events Reports System (VAERS) in the context of the gene-based modified mRNA (modRNA) prodrugs designed by Pfizer-BioNTech (BNT162b2/Comirnaty) and Moderna (mRNA-1273/Spikevax) aimed against SARS-CoV-2. Tens of thousands have reported concurrent breakthrough (BT) SARS-CoV-2 infections.
Objectives: To examine the possible link between VAERS reports of BT infection associated with the COVID-19 modified mRNA lipid nanoparticle (LNP)-encapsulated injectable products and reports of class switching toward non-inflammatory, spike-specific IgG4 antibodies especially following a third (or fourth) dose.
Methods: VAERS data was used to examine the frequency of reporting of BT infections linked to the modRNA-LNP COVID-19 products up to and including November 2024 according to dose in the “vaccine dose series” (up to dose 4), and age of the individual reporting the BT infection. Medical Dictionary for Regulatory Activities (MedDRA) Preferred Term codes “COVID-19”, “SARS-CoV-2 test positive”, “Vaccination failure”, “BT COVID-19”, "Vaccine BT infection" were used to query BT infections in the VAERS domestic dataset. These data were compared to literature-based findings indicating a shift to tolerizing (non-inflammatory) spike-specific IgG4 antibodies following third and fourth doses.
Results: There are 68,504 BT infection reports in VAERS domestic data following modRNA COVID-19 injection spanning 2020-2024 for all reports with complete age and dose 1-4 data. The highest percentage of dose-specific BT reports of total BT reports is seen following dose 4 (30%), followed by dose 3 (16%) and doses 1 and 2 (4% and 12%, respectively), even though the absolute counts of reports per dose are highest in the cases of doses 1 and 2 (N=11,330, N=31,739, N=14,999, N=10,4368, for doses 1-4, respectively). An emergent pattern in dose 4 data not seen for doses 1-3 - whereby peak reporting for 55-77-year-olds far exceeds that for doses 1-3 – was discovered following normalization of the data per 100,000 BT infection reports/age for each dose. In fact, according to Pearson Correlation, there is only a very weak correlation between doses 1 and 4 (r(97) = .45; p < .001), no correlation whatsoever between doses 2 and 4 (r(97) = .19; p = .06), and a weak correlation between doses 3 and 4 (r(97) = .58; p <.001). Doses 2 and 3 were also well correlated (r(108) = .68; p < .001). On the other hand, there is a strong significant correlation between doses 1 and 2 (r(116) = .85; p < .001) and doses 1 and 3 (r(108) = .94; p < .001). This significant difference is age-related and manifests for ages 55-77. The Area Under the Curve (AUC) for the normalized rates was calculated for dose 1 and dose 4 between the ages of 55 and 77 and the difference was found to be significant, with the dose 4 AUC being greater. Increased rates of breakthrough infection reports could be due to conferred susceptibility to SARS-CoV-2 following multiple doses of modRNA products that align with a 19.27% rise in IgG4 following dose 3 published in the literature.
Conclusions: The rates of BT reporting in the contexts of modRNA COVID-19 products are higher following dose 4 according to VAERS data. This is a compelling finding and corroborates evidence that class switching toward noninflammatory, spike-specific IgG4 antibodies confers susceptibility to COVID-19.
Keywords
SARS-CoV-2; COVID-19; modRNA; IgG4; VAERS; AUC; LNP; BT
Word Count: ____
Funding source(s): None related
Conflict of interest: Nothing to disclose. Author had access to data and wrote the manuscript.
Background
Approximately 85% of the United States population has received at least one dose of the COVID-19 injectable products and most of these were either BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna) according to CDC data as of May 10, 2023. [1,2] These products had not been fully licensed by the U.S. Food and Drug Administration (FDA) prior to August 23, 2021 [3], and were instead authorized for emergency use by the FDA under an Emergency Use Authorization (EUA) to prevent Coronavirus Disease 2019 (COVID-19). [4,5] The shots were not approved to reduce transmission or the severity of infection with SARS-CoV-2, thus any emergent AEs temporally-associated with administration of these COVID-19 shots resulting in hospitalization and death tip the risk-benefit ratio toward risk, especially considering that SARS-CoV-2 did not itself pose a risk of death in healthy and young demographics. Tens of thousands of deaths have been reported to VAERS in association with the COVID-19 shots since the roll-out began. [6] The bivalent versions of the Pfizer/BioNTech and Moderna COVID-19 injectable products were available and authorized for use in September 2022. [7]
The modRNA-LNP COVID-19 injectable products are gene-based prodrugs in that they utilize a modified messenger RNA (modRNA) as the coding material for spike protein for manufacture by “vaccine” cells delivered by the LNPs. These types of therapies have never before been deployed on such a large scale in the context of a virus. Pharmacovigilance databases such as VAERS are designed to detect safety signals in data submitted as voluntary reports of AEs in the context of pharmaceuticals or biologicals such as vaccines. [8,9] The primary purpose for maintaining the database is to serve as an early warning or signaling system for AEs not detected during pre-market testing, and has been used historically to induce the withdrawal of vaccines from the market due to observed safety issues. [10] In addition, the National Childhood Injection Injury Act of 1986 (NCVIA) requires health care providers and vaccine manufacturers to report to the Department of Health and Human Services (DHHS)[A1] specific AEs following the administration of vaccines outlined in the Act. [8,11] If safety signals emerge in the context of a particular marketed or EUDed product, such as a sudden cluster of reports of sudden death, death following cardiac arrest without known etiology or death of an infant, this would provide a reason to order and perform an autopsy. It is a criminal offense to submit a false VAERS report and can result in imprisonment. [8]
Vaccine-induced injuries or AEs can be defined as the onset of clinical symptoms that are temporally associated with vaccine/injection administration and in the absence of another known cause. [12,13] An Adverse Event (AE) is defined as any untoward or unfavorable medical occurrence in a human study participant, including any abnormal physical exam or laboratory finding from autopsy, symptom, or disease, temporally associated with the participants’ involvement in the research, whether or not considered related to participation in the research. A serious or severe adverse event (SAE) is defined as any adverse event that results in death, is life threatening, or places the participant at immediate risk of death from the event as it occurred, requires, or prolongs hospitalization, causes persistent or significant disability or incapacity, results in congenital anomalies or birth defects or is another condition which investigators judge to represent significant hazards. [8,14] The VAERS Data Use Guide states that 10-15% of reported AEs are classified as severe for any given set of data. [8]
The VAERS coding system uses an international coding system that is used worldwide called the Medical Dictionary for Regulatory Activities (MedDRA). [8, 15] The MedDRA coding system uses key words representing the AEs described in the case report and converts them to standardized codes. The MedDRA codes provided in the VAERS dataset are called the "Preferred Terms". VAERS reports are primarily filed by medical professionals (67%) and can also be filed by family members. [16] Upon individual reporting of AEs, a temporary VAERS ID number is assigned to the individual to preserve confidentiality, and a detailed description of the side effects are transcribed along with the individual’s age, residence by state, past medical history, laboratory data, allergies and sex and other details. In addition, the vax lot number, place of injection and manufacturer details are included in the report. If the VAERS report is ‘validated’ following vetting, a permanent VAERS ID is assigned, and the report is filed in the front-end data set available for download. VAERS is a prominent U.S.-based pharmacovigilance database that contains millions of reports of AEs in the context of the COVID-19 injectable products.
A BT infection is a case of illness in which a vaccinated individual becomes infected with the illness, because the vaccine has failed to provide complete immunity against the pathogen (currently only viruses). [17] BT infection reports are entered into VAERS as primary AEs when an individual succumbs to the vaccine-associated disease in the context of a pharmaceutical or biological intervention. In the case of COVID-19, a BT infection is defined by the use of a SARS-CoV-2 test that returns a “positive” result (MedDRA code “SARS-CoV-2 test positive”) reported concurrently with MedDRA codes “COVID-19”, “Vaccination failure”, “BT COVID-19” or "Vaccine BT infection". BT infections have been reported in VAERS following all doses and for the purposes of this study: from dose 1-4.
Bivalent vaccines were developed and recommended for subsequent booster doses. The bivalent Pfizer COVID-19 shot uses the Omicron BA.4 and BA.5 subvariants and the bivalent Moderna COVID-19 shot uses a mix of the original/Omicron BA.1 and Omicron BA.4 and BA.5 subvariants.[1] Although these products have been reported in the literature to be associated with BT infections, it is not an exclusive to the bivalent products and can depend on various factors, including the time since the last vaccine dose, the presence of new variants, and individual immune response.[18,19,20]
IgG4 is a subclass of antibody that responds to repeated or long-term exposure to antigens, and ‘may become the dominant subclass’ as a result of this repeated exposure. [21] Class switching to IgG4 may be modulated by Interleukin-10 (IL-10) and thus links this subclass of antibody to tolerance induction. [22] IgG4 may also represent the dominant antibody subclass in immune responses to the essential blood clotting proteins factor VIII and IX. This class switch has been found to be associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition. Individuals injected with modRNA three times who also experienced a BT infection had the highest IgG4 levels. [23]
The roll-out of COVID-19 injections are actively being monitored by regulatory agencies, but all of the risks are not yet known. [45-48] There are thousands of peer-reviewed articles documenting BT infection emergence in the context of the COVID-19 injectable products, and can be sought out by querying “vaccine-BT [infections] sars-cov-2” in PubMed.[2] [24-30]
It bears repeating that under-reporting is a known and serious limitation of the VAERS system. [8,9,31-36]
Methods
To analyze the VAERS data the Language and Environment for Statistical Computing, R was used. Excel was also used to generate the figures, to perform Pearson Correlation Coefficient calculations (significance level 0.05) and for AUC calculations. The VAERS data was downloaded as three separate comma separated values (csv) files representing i) general data for each report; ii) the reported AEs or ‘symptoms’, and iii) injection data including injection manufacturer and lot number, for each VAERS ID. In order to maximize the input variables per individual for analysis, the three files were merged using the VAERS ID as a linking variable.
For the purposes of comparing potential differences in BT infection rates with respect to doses 1 through 4, a master file was first generated containing only VAERS reports of BT infection with complete age data for the Moderna and Pfizer COVID-19 products. This was done by filtering according to “vaccine” manufacturer (VAX_MANU) (MODERNA or PFIZER\BIONTECH), filtering by vaccine dose series to ensure only data containing one of dose 1 through 4 was included (VAX_DOSE_SERIES <=4), filtering by MedDRA codes (“COVID-19”, “SARS-CoV-2 test positive”, “Vaccination failure”, “BT COVID-19” and "Vaccine BT infection"), and then finally filtering out the VAERS_IDs that did not contain age data (AGE_YRS != “NA”). Of note, to ensure that doses were not counted twice/included in sequential dose counts, only the maximum dose reported per VAERS_ID was included in the mater file. In doing so, a complete data set containing only modRNA, age-complete, dose 1-4 data was created. From this master file, four data subsets were created; each one corresponding to doses 1 through 4, by filtering by the vaccine dose series (VAX_DOSE_SERIES == 1; VAX_DOSE_SERIES ==2; VAX_DOSE_SERIES ==3; VAX_DOSE_SERIES ==4). Relevant variables were selected for each subset including VAERS ID, AEs, age, state, vaccine dose series, vaccine manufacturer and symptoms.
For each subset, the total number of BT infection reports was calculated and used to normalize the data according to each age. That is, for each specific age per dose data set, the number of BT infections was divided by the total number of BT infections per dose, and multiplied by 100,000 to obtain the normalized rate per 100,000 BT infections per age per dose. These rates were plotted for each dose and superimposed to demonstrate potential differences in trajectories according to the number of reports per age. Pearson correlation calculations were done to determine potential significant differences between doses, and AUC calculations were done specifically to demonstrate the large difference between dose 1 and dose 4 curves.
Results
BT AE reports associated with modRNA COVID-19 injectable products
As of November 2024, a total of 925,420 individuals have reported being injected modRNA COVID-19 injectable products. Of these, 702,468 have complete age data and have received either 1, 2, 3 or 4 doses. Of these, there are 93,379 (13%) domestic VAERS reports of BT infections. Of these, 68,504 (73%) have been injected with one of doses 1-4, and have age-complete data. For the purposes of this study, the data used for analysis comprised the modRNA, dose 1-4 age-complete domestic BT data (N=68,504).[3] The distributions of the absolute numbers of reports per dose and the percentage of each dose per total modRNA reports is shown in Table 1. The greatest number of BT reports is associated with dose 1 but the greatest percentage is associated with dose 4 (shown in red). In fact, almost 1/3 of all AEs reported for dose 4 are BT infection reports!

Table 1: Absolute counts for each dose (doses 1-4) in the context of all modRNA BT infection reports (BT) and modRNA total AE reports (Total). Percentages of each row total are shown in brackets. Also shown, are the percentages of each dose as per total reports of AEs (%BT/Total).
When the normalized dose data is plotted and superimposed, a clear picture of the difference in the reporting per age emerges in the context of dose 4 as shown in Figure 1. The data for doses 1 through 3 are very consistent in terms of who is filing BT infection reports in terms of age. Dose 1 is well correlated to dose 2 (r(116) = .85, p < .001) and very well significantly-correlated to dose 3 (r(108) = 0.94, p < .001). Dose 2 is likewise moderately correlated to dose 3 (r(108) = .68, p < .001). However, dose 1 is only very weakly correlated to dose 4 (r(97) = .45; p < .001) and dose 2 is not correlated to dose 4 at all (r(97) = .19; p = .06). Dose 3 and 4 also moderately correlate significantly (r(97) = .58; p < .001), even though they do not appear to from Figure 1. What is exceedingly notable from this graph - in addition to the difference in the ages reporting BT infections in the context of dose 4 - is the specificity of the ages in the yellow peak: individuals between the ages of 55 and 77 reported BT infections far more frequently following dose 4, than for doses 1-3.

Figure 1: BT infection reports from VAERS domestic data according to dose (by color) and age (x-axis) - AE count per age normalized to number of reports 100,000 BT reports/per dose (y-axis).
Many of the reports of BT infections, regardless of dose, appear to be made for individuals age 50 and older (49%, 52%, 58%, 79% for doses 1-4, respectively). This will be expanded upon in the next section. This likely has to do with incentivization strategies to “vaccinate the elderly” first, and also due to availability of products based on EUA and approval status, and to which age group these products were made available for, and when.
In order to determine the degree to which the dose 4 reports outnumber the dose 1 reports for BT infections, the AUC was calculated for dose 1 and dose 4 for the 55-77-year-old age group, and subtracted. Dose 1 and 4 were chosen as comparatives in that they are the most disparate. Figure 2 shows that the AUC is far greater for the dose 4 reports (orange), and that the difference in the AUCs between dose 4 and dose 1 when considering individuals between 55 and 77 is very large (64,766- 44,369=2,0397). This age range was selected since these ages represented the greatest discrepancy between dose 4 and dose 1. For a different perspective, there were 3,767 more reports of BT infection following dose 1 when compared to dose 4 for the 55-77 age range, however, when considering rates as per total BT infections reported per 100,000 doses, there are 20,478 more reports per 100,000 doses for dose 4 in the 55-77 age range.
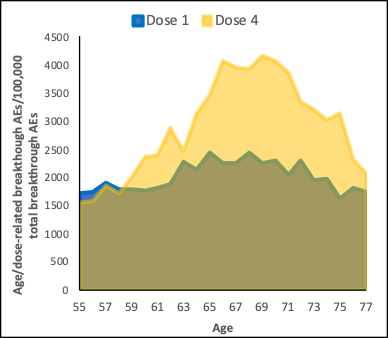
Figure 2: Visualization of the AUCs for dose 1 and dose 4 BT infection reports between the ages of 55 and 77.
Effect of bivalent products and age on BT rates
13% of dose 4 modRNA-associated reports filed to VAERS were bivalent products. This indicates that many people got the monovalent original product versions - even as fourth doses - and this could lead to BT infection depending on the variants circulating at the time. The percentages of bivalent product reports to VAERS for doses 1, 2 and 3 are 4.6%, 0.1% and 1.2%, respectively, as shown in Table 2.

Table 2: Percentages of mono- and bivalent modRNA COVID-19 products reported in the context of BT infections in VAERS.
It is possible that the bivalent products had an effect on BT infections since the highest percentage of reports were associated with dose 4 and 13% of the doses were bivalent products. It is interesting that the BT infection reports associated with bivalent products following dose 4 have two major peaks according to age in the 40s and 70s that do not occur for dose 1.

Figure 3: Absolute number of reports of BT in context of bivalent products according to age showing bi-modal pattern for dose 2 with peaks at ages 30 and 75.
The absolute counts and percentages of individuals over 50 who reported modRNA COVID-19 product-associated AEs following one of doses 1 through 4 are shown in Table 3, with the first row indicating the absolute counts and percentages of individuals who reported BT infection (per dose), and the second row indicating the absolute counts and percentages of individuals who reported any AE (per dose).

Table 3: Absolute counts (doses 1-4) and percentages in the context of two groups: i) all modRNA-associated BT infection reports (BT infection reports)) and ii) all modRNA-associated reports (All reports). The percentages of individuals 50 years of age or older in each group are shown in brackets.
The majority of individuals who succumbed to and reported a modRNA product-associated BT infection were over 50 years of age, regardless of dose (Table 2). However, 88% of the individuals who reported a modRNA product-associated BT infection following dose 4 were 50 plus, as opposed to 73% following dose 3, and 69% and 74% for doses 1 and 2. Also, 79% of the individuals who reported a modRNA product-associated general AE following dose 4 were 50 plus, as opposed to 58% following dose 3, and 49% and 52% for doses 1 and 2, respectively. The dose 4 rates in both the “All reports” group and the “BT infection reports’ group, are higher in the dose 4 context meaning that either most who received dose 4 were 50 plus and/or most succumbed to BT infections. In fact, there is a 22% and a 49% increase in reporting rate of BT infections and all AEs, respectively, when comparing dose 4 to the averages for doses 1-3.
Discussion
A large number of BT infections were caused by the Omicron variant which indicates that modRNA COVID-19 injection regimens did not confer sterilizing protection, as reported by Irrgang et al. in 2022. [23] As reported in this pivotal study, IgG4 levels sharply increased and became detectable in almost all Comirnaty vaccinees following dose 3. They also report that anamnestic IgG4 responses were seen when BT infections occurred, and were robustly detectable in the context of triple dosing before infection. It appears from their investigation that the switch is a consequence of ongoing germinal center maturation since it took a few months for the IgG4-class-switched memory B cells to appear. Their results indicate that following third and fourth doses, a class switch to a tolerizing antibody occurs and this could increase susceptibility to a subsequent SARS-CoV-2 infection with a new variant. The authors show that the observed class switch was associated with a reduced capacity of the spike-specific antibodies to mediate antibody-dependent cellular phagocytosis and complement deposition.
If one was to speculate how this might manifest with respect to pharmacovigilance reporting in a similar “real world” context, one might expect increased reports of BT infections in the context of third and fourth doses if a class-switch had occurred. Of course, this will depend on immune status at the time of injection and also previous exposures to various SARS-CoV-2 variants. It would be very interesting to know what percentage of people had prior exposure to SARS-CoV-2 in the context of BT infections. Interestingly, according to the findings of this study, increased BT infections in the context of dose 4 is precisely what was observed in VAERS. Walmsley et al. 2023 recently reported as part of a study to determine predictors of BT SARS-CoV-2 infection after vaccination, that older-aged cohorts were less likely to have a BT infections at all time-points including during the Omicron BA.4/5 and XBB waves due to establishment of hybrid immunity induced by earlier versions of the injections. [37] They concluded that the receipt of an original/Omicron vaccine was anti-correlated with BT infection, meaning that older individuals were less prone to BT infections due to the establishment of this hybrid immunity.
This is very interesting in that VAERS data in this study indicate a preponderance of BT infection reporting in older age groups, and it is likely that many of these individuals did get injected with earlier versions (ie: monovalent products) initially, and VAERS confirms this. In fact, 88% of the over 50 age group who experienced BT infection reported receiving dose 4 (modRNA product) in 2022, and the most prominently administered modRNA products in 2022 were the Pfizer and Moderna monovalent products and furthermore, according to VAERS reports, 83% of these individuals reported being injected prior to September 2022: before the bivalent products were available. Additionally, only 11% of these individuals (50+/BT/dose 4) reported being injected with a bivalent product, according to VAERS.
Also, considering that 70%, 97% and 84% of the 50 plus BT groups following doses 1, 2 and 3, respectively, were injected in 2021, it is safe to say that most of the elderly population were consistently injected with monovalent products. Only 0.05%, 0.03%, 0.18% of this group reported being injected with bivalent products following doses 1, 2 and 3, respectively. It is important to remember that because the Janssen product was used in a heterologous way - as booster to Pfizer and/or Moderna products - it would be very difficult to predict BT infection outcomes in heterologous dosing contexts – especially using VAERS data.
The administration timeframe and likely the BT infection incidence and higher reporting rates in the elderly are likely due to the preponderance of availability of modRNA COVID-19 products to older aged individuals at earlier (and all subsequent) time points during the COVID-19 injectable product roll-out, and of course, due to age-related factors such as cellular senescence and existing co-morbidities. The fact that a higher proportion of individuals who reported BT infections to VAERS had taken a fourth dose could be the result of IgG4 class-switching. It is interesting that VAERS data appears to contradict the statement made in the Walmsley et al. publication “that older individuals [are] less prone to BT infections due to the establishment of hybrid immunity induced by the earlier versions of the injections”. Again, 88% of all BT infections that were reported were made by individuals 50 years of age or more following dose 4, and 87% of these individuals reported receiving a monovalent modRNA product. In general, most of the follow-up doses were the earlier versions of the COVID-19 injectable products (monovalent), according to VAERS data. Walmsley et al. also reported “an association between higher antibody levels and protection from BT infection observed during the Delta and Omicron BA.1/2 waves of infection no longer existed during the Omicron BA.4/5 wave.” [37]
Interestingly in the Irrgang et al. study, induction of IgG4 antibodies was not observed for a non-modRNA COVID-19 injectable product (adenoviral vectors – they used Vaxzevria to examine heterologous effects; Comirnaty and the adenoviral vector–based vaccine ChAdOx1 (Vaxzevria)). As part of this study, BT infection rates were determined in the context of the Janssen COVID-19 injectable product as per VAERS reports, but since 94% of the reports (N=40,530) filed to VAERS in the context of these products were following dose 1, there isn’t much that can be said for subsequent dosing, or for subsequent dose BT infection reports. Janssen is a single dose product but it has been used as part of heterologous regimens[4], and indeed, AE (BT-inclusive) reports for non-modRNA COVID-19 products following a second, third and fourth dose have been filed to VAERS. There were a total of 4,157 reports of BT infection filed to VAERS following this non-modRNA COVID-19 injection (Janssen doses 1-4 with age complete data), whereby 90%, 9%, 0.7% and 0.3% reports were filed following doses 1 through 4, respectively.
Based on the total number of BT reports filed to VAERS as of November 2024 (N=100,545) (this is for all COVID-19 injectable products in the domestic data set), using an under-reporting factor of 31 [32], it is estimated that the actual number of COVID-19 injectable product-associated BTs in the United States is 3,116,895.
Because of the spontaneous reporting of events to VAERS, we can assume that the cases reported thus far are not rare, but rather, just the tip of the iceberg. As aforementioned, under-reporting is a known and serious disadvantage of the VAERS system. Thus, VAERS alone without adjustment, cannot be used to estimate population incidence. It is important to note that older age group reports of BT infection might be due to higher testing in these age groups (aka: “SARS-CoV-2 test positive”) or possibly that this age group may have age-related weakened immune systems.
Limitations of this study are acknowledged and are based on use of a pharmacovigilance database where reporting of AEs is voluntary. VAERS data are grossly under-reported due to many reasons, including the lack of clinical recognition of injury in the context of the COVID-19 injectable products, frustration with the VAERS online system, and fear of professional reprisal.
Conclusion
A possible link between BT infection associated with the COVID-19 modRNA products and class switching toward non-inflammatory, spike-specific IgG4 antibodies following a third (fourth) dose was investigated using VAERS domestic data. The rates of BT reporting in the contexts of modRNA COVID-19 products in VAERS are significantly higher following dose 4. This is a compelling finding, and corroborates evidence that class switching toward noninflammatory, spike-specific IgG4 antibodies confers susceptibility to SARS-CoV-2, and could be precisely why VAERS reveals a proportionally higher rate of BT infection reporting following dose 4, especially in older age groups. VAERS does come with limitations, but it is designed to emit safety signals and in the case of BT infections in the context of the modRNA shots, these signals are loud and clear. Once again, this pharmacovigilance database is functioning efficiently to reveal the signal of BT infections in the context of the COVID-19 injectable products by demonstrating – strictly via data exposure – that repeat dosing is correlated to BT infections. This subject matter bears further investigation and perhaps if these safety signals had been addressed earlier, perhaps fewer individuals may not have succumbed to BT infection potentially due to a shift to immunological tolerance from the repeat shots.
References
1. Edouard Mathieu, Hannah Ritchie, Lucas Rodés-Guirao, Cameron Appel, Daniel Gavrilov, Charlie Giattino, Joe Hasell, Bobbie Macdonald, Saloni Dattani, Diana Beltekian, Esteban Ortiz-Ospina and Max Roser (2020) - “COVID-19 Pandemic” Published online at OurWorldinData.org. https://ourworldindata.org/coronavirus
2. CDC Covid Data tracker [Internet]. Centers for Disease Control and Prevention; [cited 2023 Aug 24]. Available from: https://covid.cdc.gov/covid-data-tracker/#archived; https://data.cdc.gov/Vaccinations/COVID-19-Vaccination-Demographics-in-the-United-St/km4m-vcsb
3. https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine
4. https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19
5. FDA approved the first COVID-19 vaccine, Comirnaty (COVID-19 Vaccine, mRNA), which was previously known as Pfizer-BioNTech COVID-19 Vaccine, for the prevention of COVID-19 disease in individuals 16 years of age and older
6. https://www.openvaers.com/covid-data
7. "COVID-19 Vaccine Boosters". U.S. Food and Drug Administration (FDA). 27 September 2022; "Moderna COVID-19 Vaccines". U.S. Food and Drug Administration (FDA). 7 October 2022
8. Vaers Data Use Guide - HHS.gov [Internet]. Department Of Health And Human Services; 2020 Available from: https://vaers.hhs.gov/docs/VAERSDataUseGuide_November2020.pdf
9. Vaccine Adverse Event Reporting System (VAERS) [online]. Available at: https://vaers.hhs.gov
10. McPhillips HA, Davis RL, Marcuse EK, Taylor JA. The Rotavirus Vaccine's Withdrawal and Physicians' Trust in Vaccine Safety Mechanisms. Arch Pediatr Adolesc Med. 2001;155(9):1051–1056. doi:10.1001/archpedi.155.9.1051. https://jamanetwork.com/journals/jamapediatrics/fullarticle/191036
11. https://www.congress.gov/bill/99th-congress/house-bill/5546
12. National Research Council (US) Division of Health Promotion and Disease Prevention. Vaccine Supply and Innovation. Washington (DC): National Academies Press (US); 1985. 5, Vaccine Injury. Available from: https://www.ncbi.nlm.nih.gov/books/NBK216824/
13. https://en.wikipedia.org/wiki/Vaccine_adverse_event
14. NIA Adverse Event and Serious Adverse Event Guidelines [Internet]. [cited 2023 Aug 24]. Available from: https://www.nia.nih.gov/sites/default/files/2018-09/nia-ae-and-sae-guidelines-2018.pdf
15. https://www.meddra.org/basics
16. McLachlan, Scott & Osman, Magda & Dube, Kudakwashe & Chiketero, Patience & Choi, Yvonne & Fenton, Norman. (2021). Analysis of COVID-19 vaccine death reports from the Vaccine Adverse Events Reporting System (VAERS) Database Interim: Results and Analysis. 10.13140/RG.2.2.26987.26402
17. https://en.wikipedia.org/wiki/Breakthrough_infection
18. Andersson N.W., Thiesson E.M., Baum U., Pihlström N., Starrfelt J., Faksová K., Poukka E., Meijerink H., Ljung R., Hviid A. Comparative effectiveness of bivalent BA.4-5 and BA.1 mRNA booster vaccines among adults aged ≥50 years in Nordic countries: Nationwide cohort study. BMJ. 2023;382:e075286. doi: 10.1136/bmj-2022-075286
19. Chalkias S., Harper C., Vrbicky K., Walsh S.R., Essink B., Brosz A., McGhee N., Tomassini J.E., Chen X., Chang Y., et al. A Bivalent Omicron-Containing Booster Vaccine against Covid-19. N. Engl. J. Med. 2022;387:1279–1291. doi: 10.1056/NEJMoa2208343
20. Winokur P., Gayed J., Fitz-Patrick D., Thomas S.J., Diya O., Lockhart S., Xu X., Zhang Y., Bangad V., Schwartz H.I., et al. Bivalent Omicron BA.1-Adapted BNT162b2 Booster in Adults Older than 55 Years. N. Engl. J. Med. 2023;388:214–227. doi: 10.1056/NEJMoa2213082
21. Rispens, T., Huijbers, M.G. The unique properties of IgG4 and its roles in health and disease. Nat Rev Immunol 23, 763–778 (2023). https://doi.org/10.1038/s41577-023-00871-z
22. Akdis CA, Akdis M. Mechanisms of immune tolerance to allergens: role of IL-10 and Tregs. J Clin Invest. 2014 Nov;124(11):4678-80. doi: 10.1172/JCI78891. Epub 2014 Nov 3. PMID: 25365074; PMCID: PMC4347251
23. Irrgang P, et al. Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci Immunol. 2022 Dec 22:eade2798. doi: 10.1126/sciimmunol.ade2798. Epub ahead of print. PMID: 36548397
24. Karmacharya A, Rai K, Siwakoti S, Khanal B, Bhattarai NR. COVID-19 BT infections in vaccinated individuals at BPKIHS, Nepal. BMC Infect Dis. 2024 Sep 19;24(1):1003. doi: 10.1186/s12879-024-09902-z. PMID: 39300352; PMCID: PMC11411789
25. Nixon DF, Ndhlovu LC. Vaccine BT Infections with SARS-CoV-2 Variants. N Engl J Med. 2021 Jul 8;385(2):e7. doi: 10.1056/NEJMc2107808. Epub 2021 Jun 2. PMID: 34077640
26. Mizrahi B, Lotan R, Kalkstein N, Peretz A, Perez G, Ben-Tov A, Chodick G, Gazit S, Patalon T. Correlation of SARS-CoV-2-BT infections to time-from-vaccine. Nat Commun. 2021 Nov 4;12(1):6379. doi: 10.1038/s41467-021-26672-3. PMID: 34737312; PMCID: PMC8569006
27. Ahmad L. Implication of SARS-CoV-2 Immune Escape Spike Variants on Secondary and Vaccine BT Infections. Front Immunol. 2021 Nov 3;12:742167. doi: 10.3389/fimmu.2021.742167. PMID: 34804022; PMCID: PMC8596465
28. Ledda C, Costantino C, Motta G, Cunsolo R, Stracquadanio P, Liberti G, Maltezou HC, Rapisarda V. SARS-CoV-2 mRNA Vaccine BT Infections in Fully Vaccinated Healthcare Personnel: A Systematic Review. Trop Med Infect Dis. 2022 Jan 13;7(1):9. doi: 10.3390/tropicalmed7010009. PMID: 35051125; PMCID: PMC8781002
29. Wang R, Chen J, Hozumi Y, Yin C, Wei GW. Emerging Vaccine-BT SARS-CoV-2 Variants. ACS Infect Dis. 2022 Mar 11;8(3):546-556. doi: 10.1021/acsinfecdis.1c00557. Epub 2022 Feb 8. PMID: 35133792; PMCID: PMC8848511
30. Nguyen M, Paul E, Mills PK, Paul S. Risk of COVID-19 Reinfection and Vaccine BT Infection, Madera County, California, 2021. Am J Epidemiol. 2024 Aug 27:kwae308. doi: 10.1093/aje/kwae308. Epub ahead of print. PMID: 39191647
31. Rose J. A Report on the U.S. Vaccine Adverse Events Reporting System (VAERS) of the COVID-19 Messenger Ribonucleic Acid (mRNA) Biologicals. Science, Public Health Policy and the Law. 2021 May 01; v2.2019-2024
32. Rose, J. 2021, Critical Appraisal of VAERS Pharmacovigilance: Is the U.S. Vaccine Adverse Events Reporting System (VAERS) a Functioning Pharmacovigilance System? Science, Public Health Policy & the Law Volume 3:100–129. https://dx.doi.org/https://www.publichealthpolicyjournal.com/
33. Lazarus, Ross et al. Grant Final Report. Grant ID: R18 HS 017045. Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS). Submitted to The Agency for Healthcare Research and Quality (AHRQ). https://digital.ahrq.gov/sites/default/files/docs/publication/r18hs017045-lazarus-final-report-2011.pdf
34. Hodel KVS, Fiuza BSD, Conceição RS, Aleluia ACM, Pitanga TN, Fonseca LMdS, Valente CO, Minafra-Rezende CS, Machado BAS. Pharmacovigilance in Vaccines: Importance, Main Aspects, Perspectives, and Challenges—A Narrative Review. Pharmaceuticals. 2024; 17(6):807. https://doi.org/10.3390/ph17060807
35. García-Abeijon, P.; Costa, C.; Taracido, M.; Herdeiro, M.T.; Torre, C.; Figueiras, A. Factors Associated with Underreporting of Adverse Drug Reactions by Health Care Professionals: A Systematic Review Update. Drug Saf. 2023, 46, 625–636
36. Zhou W, Pool V, Iskander JK, English-Bullard R, Ball R, Wise RP, Haber P, Pless RP, Mootrey G, Ellenberg SS, Braun MM, Chen RT. Surveillance for safety after immunization: Vaccine Adverse Event Reporting System (VAERS)--United States, 1991-2001. MMWR Surveill Summ. 2003 Jan 24;52(1):1-24. Erratum in: MMWR Morb Mortal Wkly Rep. 2003 Feb 14;52(06):113. PMID: 12825543
37. Walmsley S, Nabipoor M, Lovblom LE, Ravindran R, Colwill K, McGeer A, Dayam RM, Manase D, Gingras AC, On Behalf Of The STOPCoV Team. Predictors of BT SARS-CoV-2 Infection after Vaccination. Vaccines (Basel). 2023 Dec 28;12(1):36. doi: 10.3390/vaccines12010036. PMID: 38250849; PMCID: PMC10820583
[1] https://en.wikipedia.org/wiki/Moderna_COVID-19_vaccine
https://pubmed.ncbi.nlm.nih.gov/?term=vaccine-BT+sars-cov-2
[3] This is one of the limitations of VAERS: not all variable fields are occupied with data due to poor transcription of reports leading to incomplete reports.
[4] https://en.wikipedia.org/wiki/COVID-19_vaccine_clinical_research#Heterologous_prime-boost_vaccination
[A1]Spell out the meaning of the acronym.
Can we safely say that the more inoculations of this garbage. The more it weakens the immune system.
Nobel laureate Luc Montagnier did warn that everyone who got the jabs should be tested for AIDS and that a large percentage would be dead in 5 years.