


In response to the December 13, 2021 ACIP meeting presentation by John Su
Things are not as they are being presented.

Update: I have removed any possible non-COVID-19-associated VAERS IDs. See updated slides. The ‘possibility’ that they are is not good enough for me: I need to know that they are.
David Wiseman is the guy on top of secret ACIP meetings and wrote to me this morning and asked me to confirm/deny what John Su presented in his most recent presentation “Adverse events among children ages 5-11 years after COVID-19 vaccination: updates from v-safe and the Vaccine Adverse Event Reporting System (VAERS)”. I was aware of the meeting the day it happened - this is one of their new techniques: have the meetings and don’t announce them so that no one has any bloody time to prepare and present counter data to them.
The first figure here refers to the title slide of this fantastic presentation.

As my readers may already know, I am only analyzing the VAERS Domestic data so I selected the slides in John Su’s slide deck that refer to VAERS descriptive statistics. His data refers to VAERS reports on or before December 10, 2021 and my data refers to December 17, 2021. I decided to pick the following week’s update to further isolate signal discrepancies.
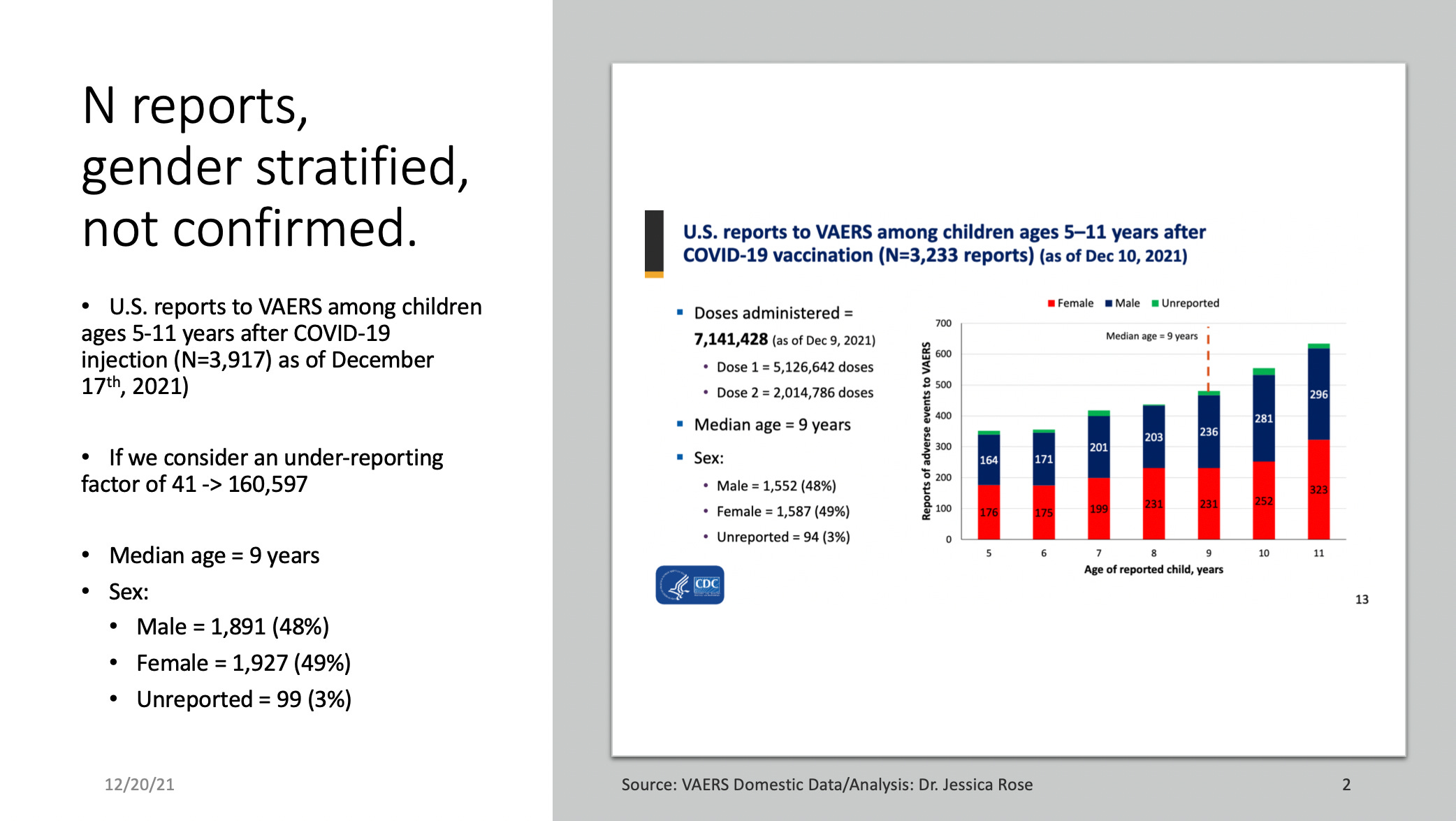
The first slide is as follows and presents the total number of adverse event reports for children ages 5-11 submitted to VAERS as of December 10, 2021. The first thing to notice is the N which is N = 3,233. This count is 68% lower than the actual N following merging the 3 .csv Domestic Data files downloaded from the VAERS website. The value of N following file merging is N = 5,430. He got the median age right, however, and the percentage distribution among gender. Amazing.
The next slide shows the distribution of the reports with respect to temporal proximity to injection date. The trend is well presented but the numbers are wrong. 88% of reports were filed within 24 hours. This is also a point of extreme interest that I have previously published here on Substack.

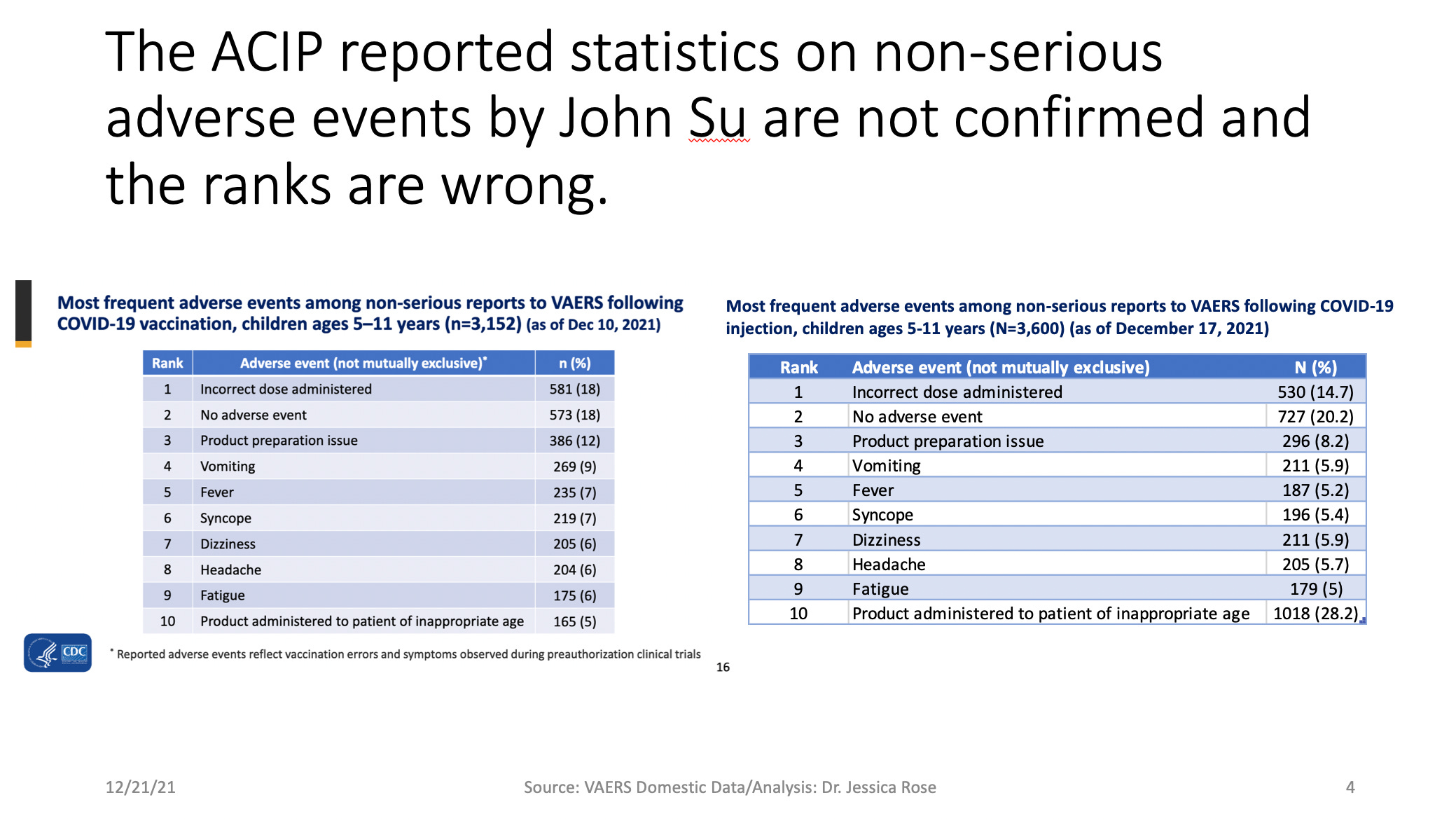
The next slide shows the top 10 reported adverse events among non-serious reports filed to VAERS following COVID-19 injection in children ages 5-11 as of December 10, 2021. As you can see, when Symptom 1 is selected (there are 5 Symptom columns), John mysteriously buries “Product administered to patient of inappropriate age” at position #10 when it is, and has been at position #1 since the very beginning of the roll out and subsequent entries filed to VAERS for this age group. I presented this to the VRBPAC/FDA hearing concerning 5-11 year olds. They know about it. And they are hiding it. In bloody plain sight. If you don’t understand the implications of this think of it this way: the most commonly-reported MedDRA code in VAERS for children 5-11 is that they were injected without having been asked how old they are first. There are 1,018 reports of injections into children of the wrong age - not 165. And by the way, is this really not considered a serious report? Oops, I injected this baby by mistake. I thought they were 7! It’s probably not this bad but the point is the same. Why are the guidelines so loose and fast here? Why was it even possible for a 9 year old boy from Florida to get injected TWICE in June? What the hell is going on here? Seriously?
(No URF considered here.) I mean, think about it! These are alleged trained medical professionals administering these shots, as a reminder. The N for children who reported non-severe adverse events is N = 3,917, not N = 3,152. The actual top 10 non-serious adverse events are different form what John Su presents here. Talk to me if you want the list.
The next slide shows the same list of top 10 reported severe adverse events among reports filed to VAERS following COVID-19 injection in children ages 5-11 as of December 10, 2021. These Symptoms are the MedDRA coded adverse event reports associated with hospitalizations, emergency room visits, death, life threatening issues, birth defects or disabilities. The total number of children aged 5-11 who reported a severe adverse event is N = 317. This number is far larger than John’s whereby his is N = 81. The top 10 severe adverse events are not even close to the top 10 that John Su presents here. Where the hell is myocarditis, for example? And why does he use the term ‘Fever’? The MedDRA code for ‘fever’ is ‘Pyrexia’. If you do a search for the number of fever reports using VAERS, you need to use the MedDRA coded term ‘Pyrexia’.

The other thing I cannot figure out is where John got his 10 Troponin increased counts from. There are 2. I checked. Which I also find questionable. But, my purpose in this exercise was simply to see if I could reproduce his slides (and I could not). So I will leave it at that and not speculate at this point.
You guys should also know that nightmares and sleeping disorders are notable adverse event reports for these children and this is extremely concerning. No sleep = no immune system optimization. There are also 128 reports classifying as mental disturbances including ‘Hallucinations’ and ‘Aggression’.
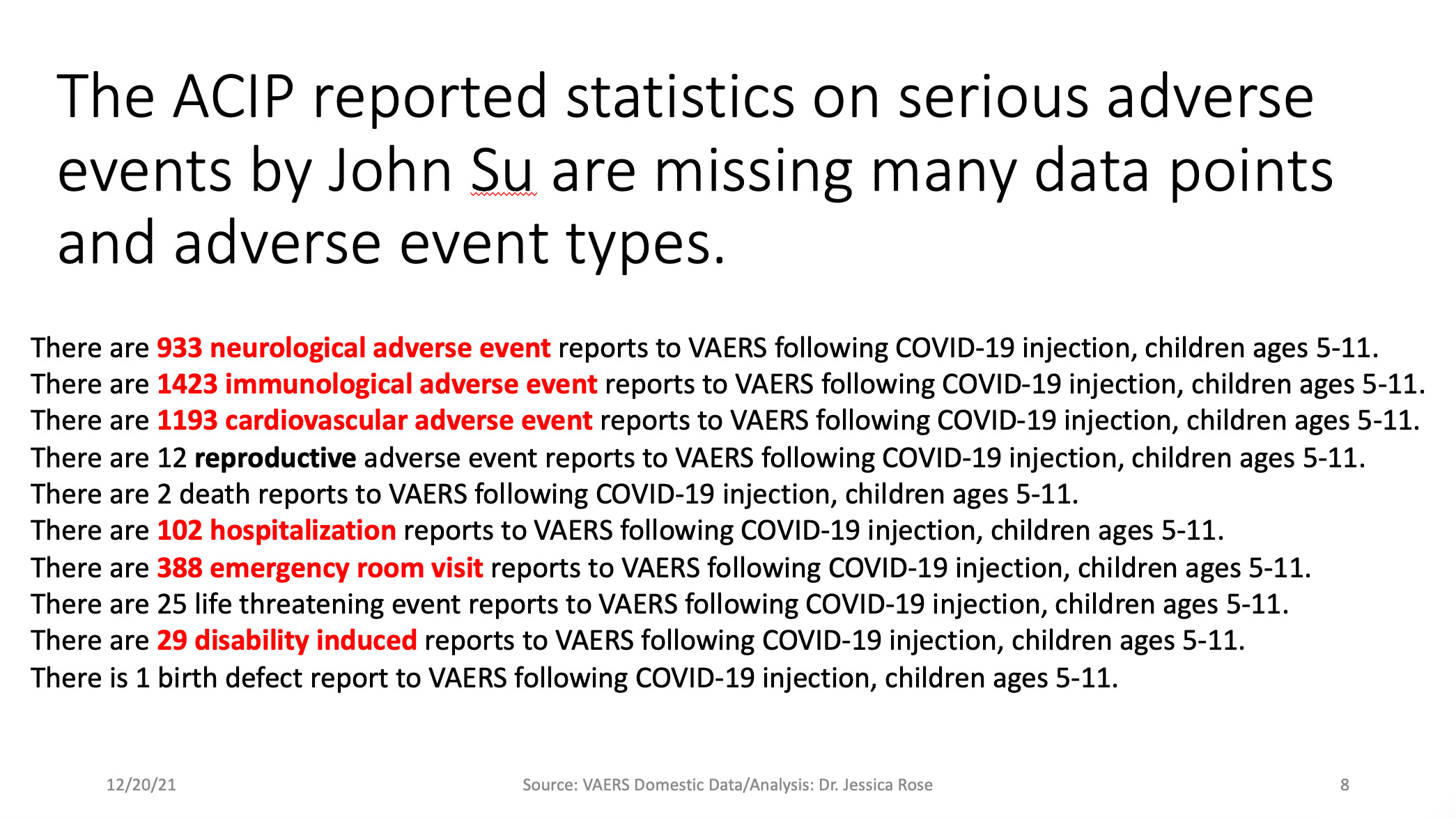
The next slide shows some more descriptive statistics regarding the severe adverse events that John failed to mention in his presentation. I group the MedDRA coded adverse event reports according to cardiovascular, neurological, immunological or reproductive involvement/description. The Ns associated with each group is shown as follows and indicates that neurological, immunological and cardiovascular adverse events are being reported at 18, 28 and 23 reports per 100,000 children according to Dose 1 rates (5,126,642) listed in slide 2 above, and 13, 20 and 17 reports per 100,000 children according to the total number of doses (7,141,428).
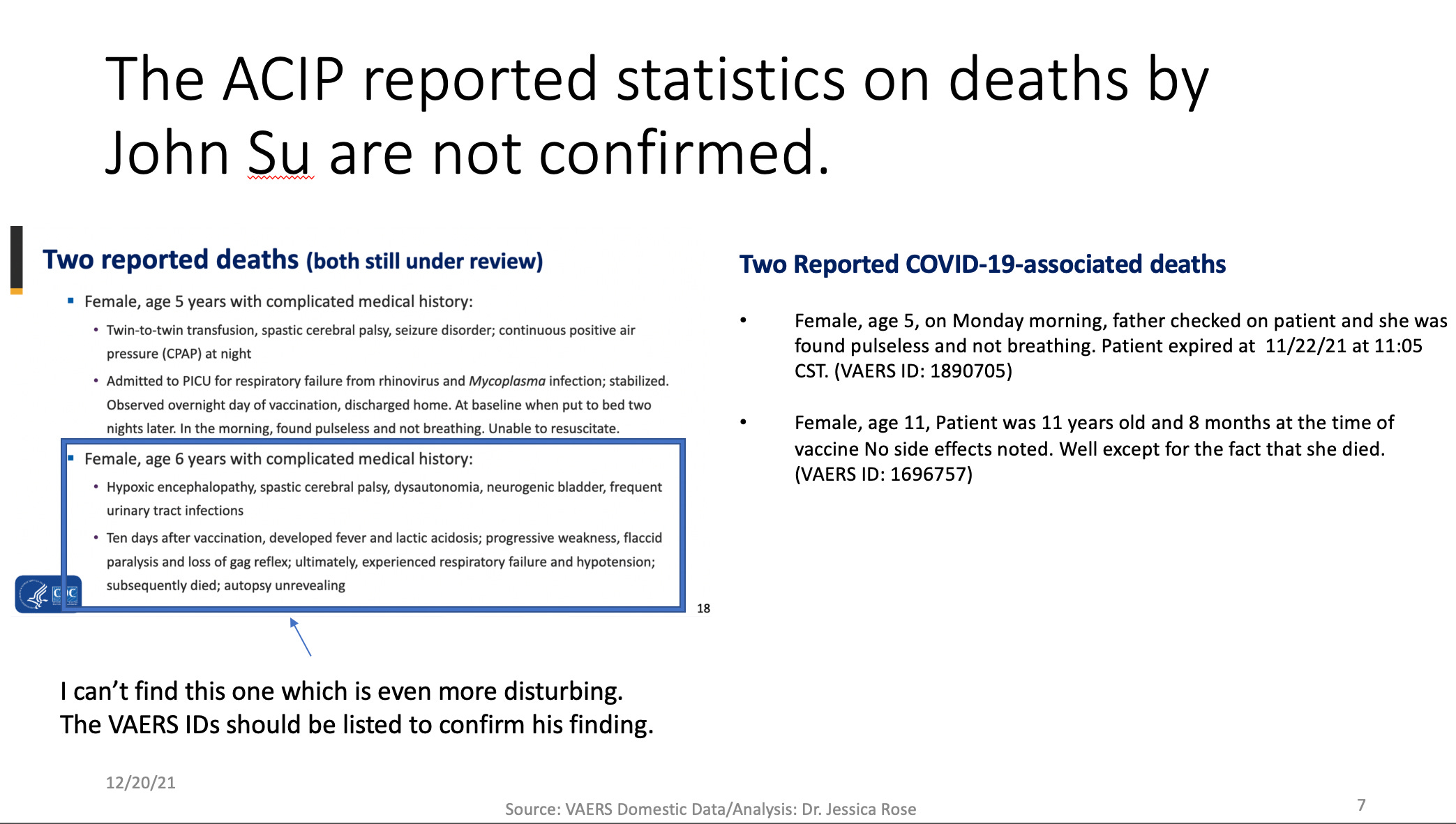
The next slide shows the actual reported deaths in the 5-11 year old age group in VAERS. It is very strange to me that I could not locate the 6 year old little girl that he reports in his presentation. However, as I have reported previously, there is an 11 year old little girl who died in association with the Pfizer injections and she is not presented here by John Su. Seems like more than a minor oversight. There are 3 additional deaths in this age group with missing injection manufacturer data so although it is possible that they died in association with other products, it is also possible that they died in association with the COVID-19 products. In any case, they are dead shortly following whatever injections they got. That data shouldn’t be missing. (Note these 3 have been officially omitted from this assessment since they are not confirmed COVID-19-related reports.)
And finally, everyone’s favorite childhood injection injury: myocarditis. I use the keywords listed on John Su’s list from his previous presentation when I do my myocarditis queries. I also include “Chest pain” since it is associated (96.1% of the time according to Fazlollahi et al.) with injection-induced myocarditis in almost every instance.1 2 3 4 5
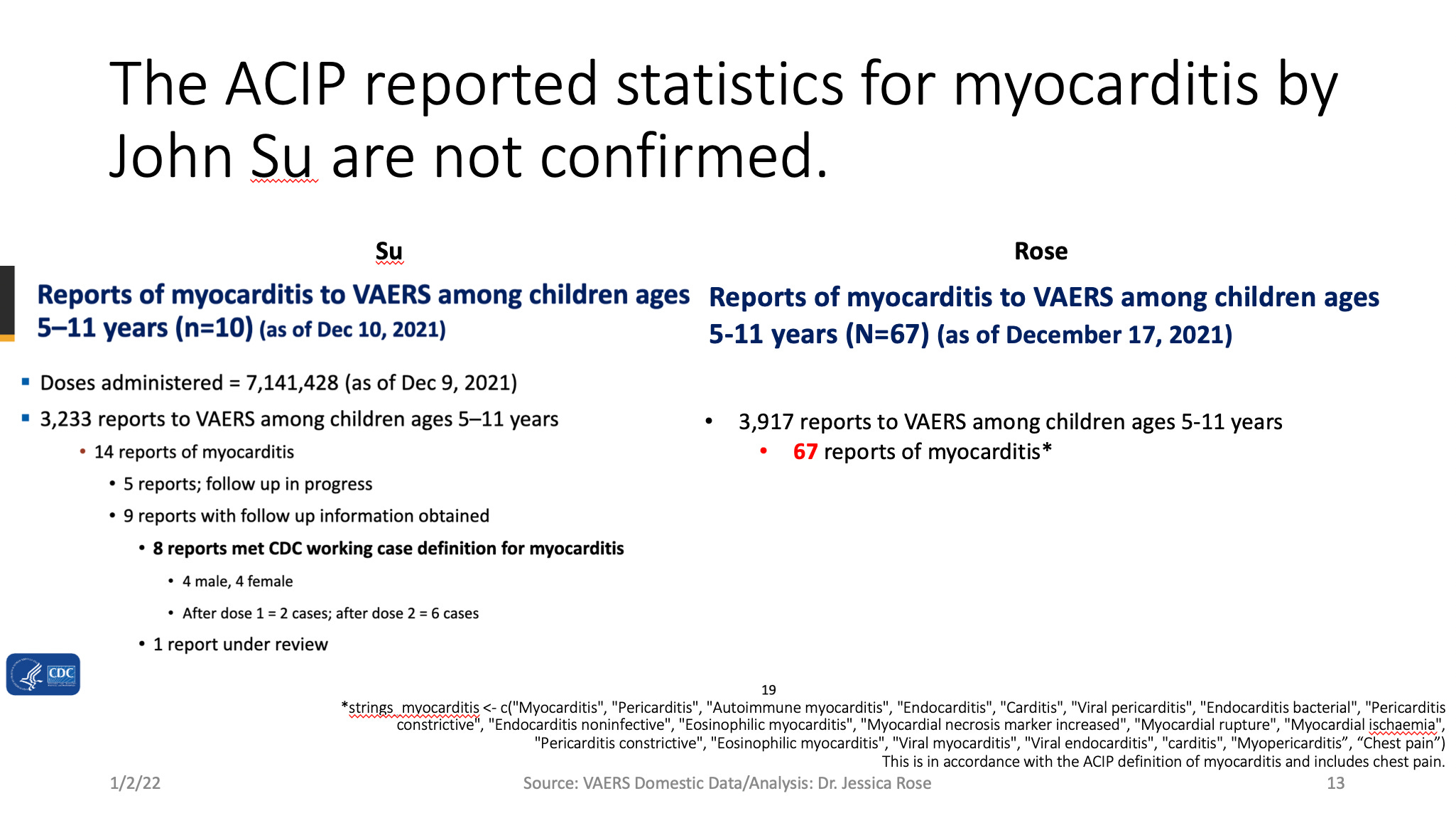
So John’s myocarditis count is off as well. When “Chest pain” is considered as a diagnostic marker of myocarditis in 5-11 year olds, N = 67. When I remove the keyword “Chest pain”, my myocarditis count is N = 5. This bothers me. Even though my N is lower, the question becomes: WHY? Where are the other 5 cases and what are their VAERS IDs?
This has been a quick and dirty direct comparison of what has most recently been presented by an ‘expert’ to the FDA panel of judges who are in charge of deciding whether or not it is a good idea to inject, and to keep injecting little kids with this crap. I have presented what is actually present in the front-end VAERS Domestic dataset.
Big thanks to David (and everyone else) for persistent and hard work. :)
Matta A, Kallamadi R, Matta D, Bande D. Post-mRNA COVID-19 Vaccination Myocarditis. Eur J Case Rep Intern Med. 2021;8(8):002769. Published 2021 Aug 16. doi:10.12890/2021_002769
Park J, Brekke DR, Bratincsak A. Self-limited myocarditis presenting with chest pain and ST segment elevation in adolescents after vaccination with the BNT162b2 mRNA vaccine. Cardiol Young. 2021 Jun 28:1-4. doi: 10.1017/S1047951121002547. Epub ahead of print. PMID: 34180390.
Singh B, Kaur P, Cedeno L, Brahimi T, Patel P, Virk H, Shamoon F, Bikkina M. COVID-19 mRNA Vaccine and Myocarditis. Eur J Case Rep Intern Med. 2021 Jun 14;8(7):002681. doi: 10.12890/2021_002681. PMID: 34268277; PMCID: PMC8276934.
Dionne A, Sperotto F, Chamberlain S, Baker AL, Powell AJ, Prakash A, Castellanos DA, Saleeb SF, de Ferranti SD, Newburger JW, Friedman KG. Association of Myocarditis With BNT162b2 Messenger RNA COVID-19 Vaccine in a Case Series of Children. JAMA Cardiol. 2021 Dec 1;6(12):1446-1450. doi: 10.1001/jamacardio.2021.3471. PMID: 34374740; PMCID: PMC8356143.
Fazlollahi A, Zahmatyar M, Noori M, Nejadghaderi SA, Sullman MJM, Shekarriz-Foumani R, Kolahi AA, Singh K, Safiri S. Cardiac complications following mRNA COVID-19 vaccines: A systematic review of case reports and case series. Rev Med Virol. 2021 Dec 17:e2318. doi: 10.1002/rmv.2318. Epub ahead of print. PMID: 34921468.
Unbelievable! Amazing work on this; they need to be held accountable.
Jessica, your work is EXCELLENT, and I love your passion, as well. I happened to catch you just yesterday on an interview with Dr. Mercola — at the time I didn’t realize you were the same person (I hadn’t paid much attention to your name at the time) as the one here on substack here that I was subscribed to.... I’m delighted that you are one and the same!! I resonated with everything you said in the interview, you beautiful woman you, especially the part about how not being able to move your body (since you love surfing every day) could be a fate worse than death for you. And how you (and others) find ways to circumvent the orders to get out of the water and/or outrun the guards. SO GLAD YOU EXIST IN THIS WORLD AND ARE DOING THE WORK THAT YOU DO!!!!