


IgG4-related disease (IgG4RD) means FIBROSIS and organ destruction
That leads to death, eventually...

Let’s get some definitions out of the way:
Fibrosis is a pathological wound healing in which connective tissue replaces normal parenchymal tissue to the extent that it goes unchecked, leading to considerable tissue remodeling and the formation of permanent scar tissue.1
Connective tissue is one of the four primary types of animal tissue, along with epithelial tissue, muscle tissue, and nervous tissue.2
Collagen is the main structural protein in the extracellular matrix found in the body's various connective tissues.3
Type I collagen is the most abundant collagen of the human body. It forms large, eosinophilic fibers known as collagen fibers. It is present in scar tissue, the end product when tissue heals by repair, as well as tendons, ligaments, the endomysium of myofibrils, the organic part of bone, the dermis, the dentin, and organ capsules.4
Type III collagen is one of the fibrillar collagens whose proteins have a long, inflexible, triple-helical domain. Type III collagen is found as a major structural component in hollow organs such as large blood vessels, uterus and bowel.5
A recent paper published in Science confirms what many of us have been saying for well over a year now: repeated injections with modified mRNA encapsulated by LNPs messes up your immune system.
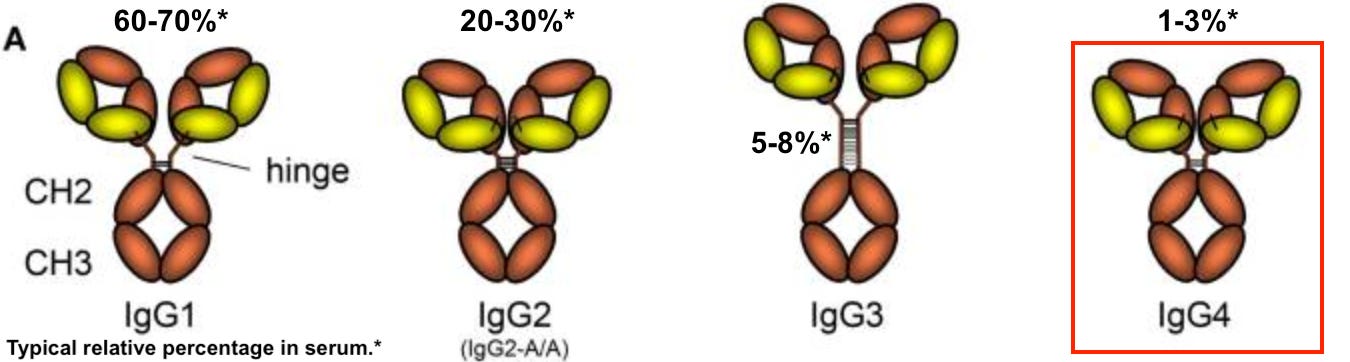
It messes it up in a specific way. We have evidence from this work that the fibrosis and organ destruction we are witnessing in countless numbers of folks post COVID injection, is due to the shots and more specifically, likely due to the eventual class switching to IgG4 and subsequent prevalence (perhaps dominance) of this antibody subclass. Just so that you know, the typical relative percentages of the four subclasses of IgG in the blood are the following: 60-70% IgG1, 20-30% IgG2, 5-8% IgG3, 1-3% IgG467.
So if IgG4 percentages are much higher than 1-3% in the blood, then something is out of the ordinary. It may even manifest pathologically. To reiterate from my last Substack article, the authors found a 48,075% increase (from 0.04% - 19.27%) in spike-specific IgG4 antibodies in test subjects between the 2nd and 3rd injections of the Comirnaty product, so I suppose this would translate to a presence of IgG4 in the blood at levels higher than 1-3%. Probably closer to 20%? In any case, the shift in IgG subclass ratios is notable following the 2nd and 3rd injections.
Before I dig into IgG4RD, I want to make something clear. The role of IgG4 as a ‘tolerizing antibody’ is inherently linked to T regulatory cells (Tregs) - the immune ‘tolerancers’: IgG4 is not directly responsible for tolerization. This means that IgG4 is not so much the tolerizer, as it is a medium for tolerization via Tregs. I think calling it a tolerizing antibody is appropriate. I have provided background on Tregs in a previous Substack, but I will give a very quick summary here of their role in immunological tolerance - and also what immunological tolerance is!
Immunological tolerance is the process of making sure that your immune system doesn’t turn on you. Imagine if you didn’t have a system in place to ensure that your immune cells only recognized foreign antigens as bad guys? Imagine what would happen, therefore, if your immune cells recognized your antigens as bad guys? Maybe… autoimmunity?
An antigen (Ag) is a molecule that can bind to a specific antibody or T-cell receptor. Antigens can be proteins, peptides (amino acid chains), polysaccharides (chains of monosaccharides/simple sugars), lipids, or nucleic acids.8
Immunological tolerance happens in the thymus and involves removing potentially self-reactive T cells (and B cells in the bone marrow) such that they do not have the eventual ability to act on self antigens, because they are removed. The effect of this in the living being, for example, is a lack of systemic and persistent autoimmunity. In my opinion, when faced with the onset of an autoimmune condition, one must think ‘out-of-balance Treg population’ - either quantitively or qualitatively.
One more thing on Tregs. There are natural and induced Tregs. Natural Tregs originate from the thymus (central) with a FoxP3+ phenotype. All this means is that they are ready to go as immunological tolerizers when they exit the thymus, ie: when they meet ‘auto-reactive’ cells in the periphery, they say ‘hasta la vista, baby’, to them. Induced Tregs include naïve T cells circulating in the periphery (peripheral) that can be induced to differentiate to the Treg phenotype to act out all the effector functions of a Treg (maintaining non-responsiveness to self-antigens) - even though they are different from natural Tregs. This is important to understand for the coming points made in this article.
Again, Tregs are essential to the maintenance of immunological unresponsiveness to self-antigens thus protecting the host from unwanted immunological responses to self.
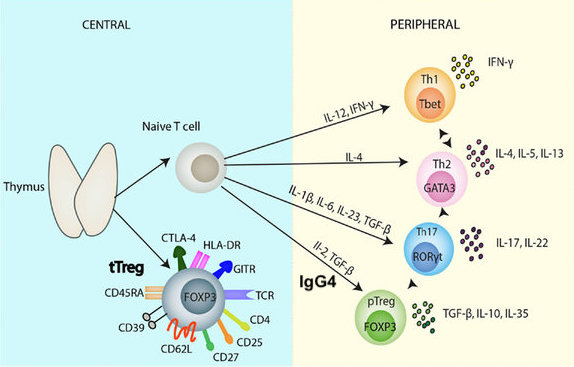
The role of IgG4 in Treg differentiation is made clear in a paper that I will discuss in the following paragraphs. But just so that you’re not in suspense, according to their findings, IgG4 induces a Treg phenotype switch in the periphery - from naïve to Treg, and thus modifying the ratio of Tregs to T helper type 1 and 2 (Th1/Th2) cells, for example, and all of the subsequent effects that follow.
Now that we know how important Tregs are and their role in preventing autoimmunity and how they are linked to IgG4, let’s now dig into IgG4 disease or IgG4-related disease (IgG4RD). IgG4RD mainly affects middle-aged to elderly men.9 Its clinical symptoms are relatively mild, and the condition usually comes to clinical attention due to swollen organs or even organ damage. Many patients with IgG4RD respond very well to steroid therapy, but without treatment, this disease is fatal.10 A paper published in 2014 revealed death by IgG4RD involvement by coronary artery occlusion by thrombosis.11
In my research, I found many papers covering IgG4RD subject matter from all around the world: it is most certainly a well-studied, albeit emerging ‘disease’. It’s more like a bunch of diseases that involve IgG4. Diseases such as Mikulicz’s disease, Sjögren’s syndrome and autoimmune pancreatitis (AIP) are all linked to IgG4. If you’re interested, there are multiple studies from Japan, the United States (ongoing research [facility] in Boston), Taiwan, Mexico, Italy, and China that I found.121314151617
One of the papers that came out of China - which was brought to my attention today by Stephanie Seneff - really got my attention. It is entitled: “The role of PD-1/PD-Ls in the pathogenesis of IgG4-related disease”, published in Rheumatology in 2021.18 The reason this particular paper caught my attention, and kept it, is because the authors provide evidence that IgG4RD is linked to the promotion of differentiation of naïve T cells (in the periphery) to a Treg phenotype via a programmed cell death protein/ligand interaction. What does this mean? It means IgG4RD → more Tregs → more IL-10/TGF-beta → more IgG4 → more IgG4RD → more fibrosis, etc192021… With just about everything related to immunology, to solve the chicken and the egg problem, is a difficult task. I will return to this soon.
It is interesting to me that the Boston crew referenced above are testing out a therapy called rituximab: a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of B cells. You may be surprised to know that when it binds to this protein, the B cell dies.22 Even more interestingly, an article published in The Lancet in December 2021 reported that using rituximab is a bad idea in the context of COVID-19 in terms of disease severity. I tend to agree with The Lancet, in this particular case. Rituximab can cause cardiac arrest, cytokine storm and pulmonary toxicity, to name a few adverse events, on its own. You’ll all be happy to know that it’s on the WHO's list of essential medicines. So is Ivermectin!23
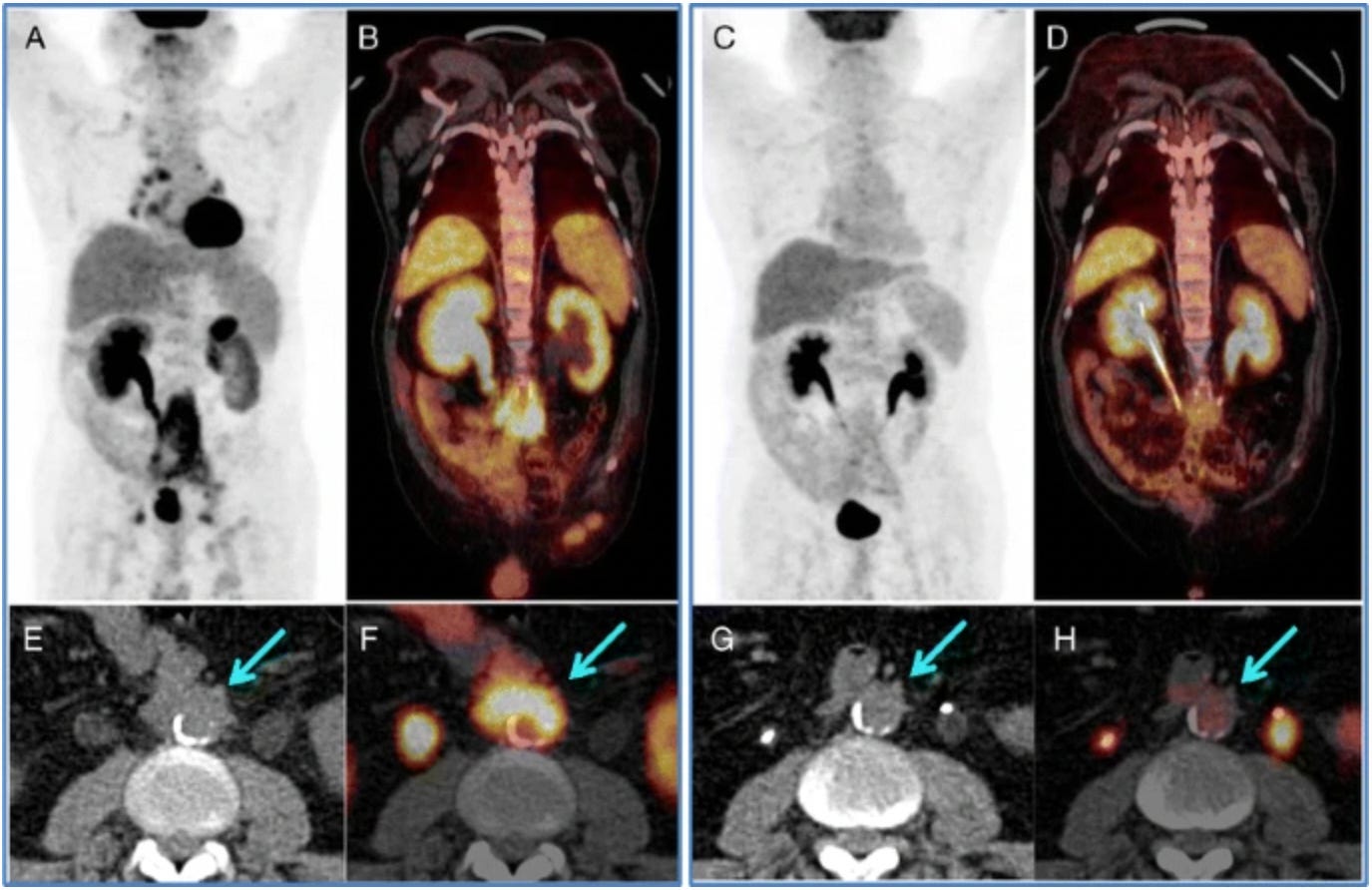
There are quite a few pathologies associated with IgG4RD, but they all involve the fibro-inflammatory processes inherent to it. Figure 3 shows an example of one of these manifestations, namely retroperitoneal fibrosis with aorta involvement, from a paper published in 2014 characterizing IgG4-related disease using PET/CT methods.24
As previously mentioned, IgG4RD becomes clinically-evident due to organ swelling and can be remedied with steroid therapy. Diagnosis can be confirmed with histopathology, or treatment alone, if you happened to be House, MD. This disease can indeed affect a multitude of organs and has organ-specific diseases named accordingly affiliated with the pancreas, the lungs, the bile ducts, the kidneys, the meninges, the lacrimal (tear) glands, the thyroid, the lymph nodes, the peritoneum or retroperitoneal tissues (abdomen) and… the aorta.
The aorta, eh? I want to know more about that. I found a paper entitled: “Aortitis, periaortitis, and retroperitoneal fibrosis, as manifestations of IgG4-related systemic disease”.25 The folks who penned this paper wrote:
IgG4-related systemic disease should be considered in any patient found to have aortitis (or periaortitis).
Really? Ok. I am curious as to what VAERS reveals. Let’s do a search for Aortitis. I doubt I will find any reports, but let me see. There are N = 36 reports in VAERS for Aortitis. This surprised me. A lot. What doesn’t surprise me is that over the past 5 years, there is only a single report of Aortitis filed in 2020 associated with the shingles vaccine VARZOS, in VAERS. So my next question is, if these authors are correct in their assessment that IgG4RD should be considered in any person found to have Aortitis, then shouldn’t these people who filed VAERS reports be followed up for presence of IgG4 antibodies to confirm or deny IgG4RD? I smell a FOIA request coming!
Noninfectious thoracic aortitis, periaortitis and idiopathic retroperitoneal fibrosis have all been linked to IgG4RD, according to their findings. Noninfectious aortitis refers to disorders that involve chronic inflammation within the aortic wall and importantly, can manifest from giant cell arteritis, rheumatoid arthritis, ankylosing spondylitis and Behçet's syndrome/disease (this might interest you, Retsef).
I looked for these as stand-alone adverse event reports in VAERS because two independent researchers that I know, and also a heap of people by email, have asked me about giant cell arteritis and Behcet's. This can't be a coincidence. They asked me for a reason based on something they were seeing; presumably in personal, clinical or lab research.
There are N = 432, 3,025, 368 and 78 cases of giant cell arteritis, rheumatoid arthritis, ankylosing spondylitis and Behçet's syndrome, respectively. As a group of reported adverse events, 34% of these reports followed dose 2, and 15% followed dose 3. With regard to modified mRNA manufacturers, 73% are associated with Pfizer and 23% are associated with Moderna.
Here’s a good article describing the manifestations of IgG4RD according to organ systems and blood.26
This is the paper to rule them all - well, for this Substack article anyway. It is entitled: "Immunology of IgG4-related disease".27 It is incredibly insightful on the subject matter of the fibrotic aspects of IgG4RD, and this fibrosis thing is really interesting to me since we have yet to nail down whether or not people are succumbing to amyloidosis from the production of amyloids from spike, or from excessive fibrin production due to impairments in the clotting pathway or from excessive collagen production and deposition due to exacerbated (genetic) defects. This is all in the context of the COVID shots, of course. I want to remind everyone here though that IgG4RD is not the same thing as spike-specific IgG4-mediated spike tolerance. Thanks for commenting on 'Twitter', Jikkyleaks. Good point to make here indeed!
They write:
…aberrant T helper type 2 (Th2)/regulatory T cells sustained by putative autoreactive B cells have been proposed to drive collagen deposition through the production of profibrotic cytokines...
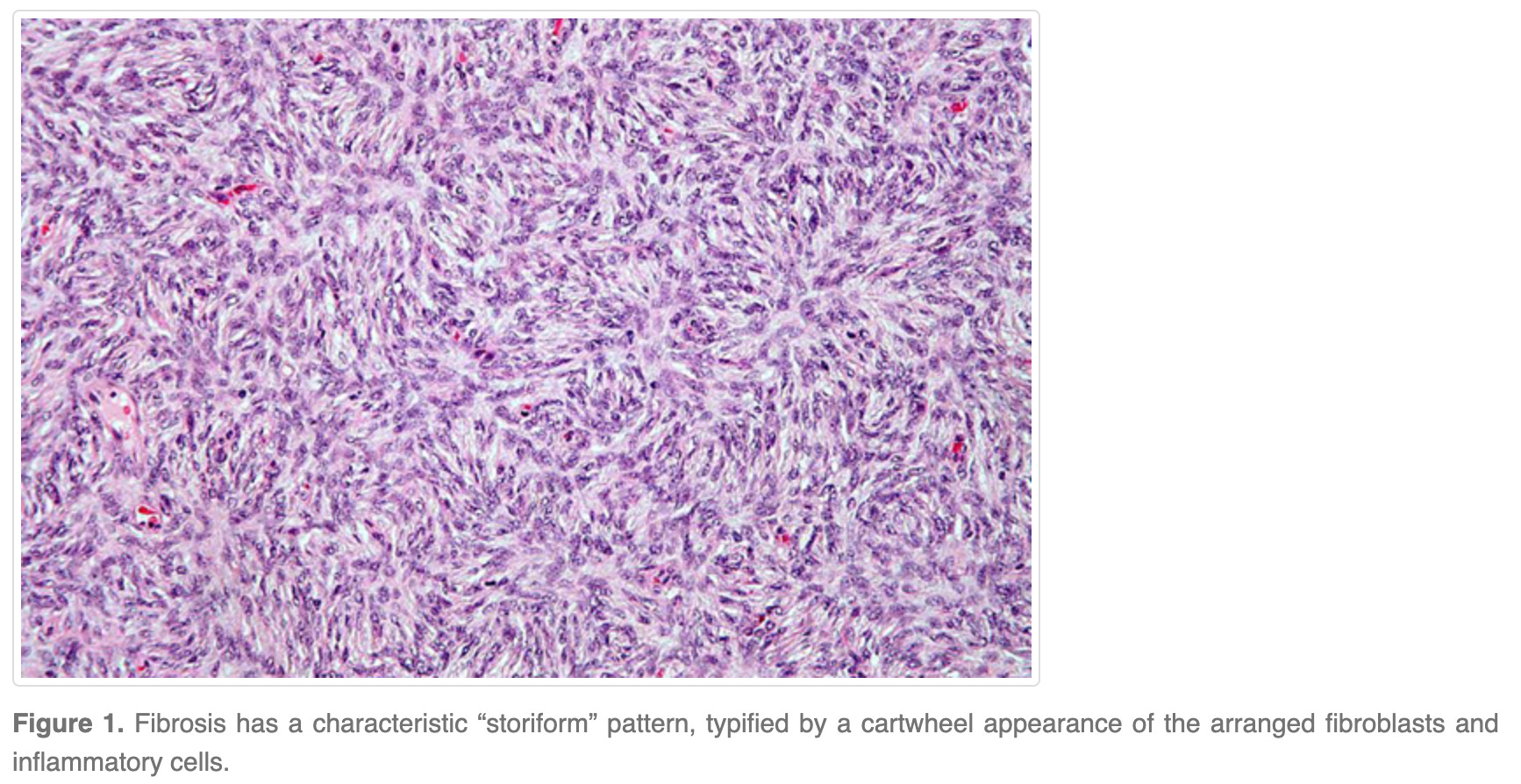
There is hallmark of IgG4RD called ‘storiform fibrosis’ which refers to an irregularly ‘whorled’ organization of collagen bundles.28 A collagen bundle looks like twisted licorice so imagine an irregularly whorled version of twisted licorice inside your body. If you’re in the lab looking for stuff going wrong from people who died in temporal proximity to getting these COVID injections, look for this.
Now, there’s a reason why I defined Type III collagen in the list of definitions at the beginning of this article. It’s because they are a major structural component in large blood vessels. There’s a particular connective tissue disease cluster that has piqued my interest of late called Ehlers-Danlos syndromes (EDS) and incredibly, I found out today that besides being exceedingly rare (~1/100,000 cases reported in the U.S.2930 or less rare: 1/1,667 for hypermobile EDS in the U.S.31) and inherited, it is the result of a gene defect causing improper Type III collagen production. And what is even more interesting is that there are 23 reports of EDS in VAERS in the context of the COVID shots (Janssen, Moderna and Pfizer) as of December 23, 2022. There have been 2 reports filed to VAERS in the past 5 years, which stuns me. These were reports where a history of EDS was not reported. They were filed in 2017 and 2018 in the context of the HPV (Guardasil) and influenza (FLUA3) products.
To me, there shouldn’t be any reports of EDS in VAERS at all, except if it’s written up in the history. Otherwise, it would appear as though the syndrome is a result of the product that the person is writing the VAERS report for. The typical age of manifestation of clinical signs is infancy, for EDS. In the case of hypermobile EDS, it can manifest at any age. The respective ages of the reports filed in 2017 and 2018 are 27 and 18. In the latter case the reporter wrote that the EDS manifested 5 months after vaccination and in the former case, the reporting gynecologist wrote that hypermobile EDS was suspected as diagnosis for this 27-year old woman, who initially reported cluster headaches and polycystic ovary syndrome.

Just to finalize this point of potential causative effects, the average age of the 23 cases of reported EDS (and hypermobile EDS) (without reported history) in VAERS in the context of the COVID-19 products is 35, with the youngest report filed for a 12 year old. At least 5 of these have reported hypermobile EDS development/onset associated with their injection but I suspect, they all are hypermobile EDS cases since none of them are reported in the history and manifested post infancy.
It strikes me to this day how a handful of intussusception cases in VAERS in 1999 resulted a causality assessment of ‘very likely’, that in turn resulted in the Rotavirus vaccine being pulled from the market. How is it possible that a handful (23) of cases of something like (hypermobile) EDS associated with these COVID injectable products is not prompting the same action? There might be no causal effect, but what if there is? Wouldn’t we want to know?
But EDS and causation are not what I want to focus on, for now. I would like to redirect to Type III collagen deposition in large blood vessels. This reminds me of something, and gets me back to why I started researching connective tissue disorders 3 weeks ago, in the first place. These rubbery, proteinaceous deposits that embalmers are claiming to be pulling out of cadavers (I haven't seen this with my eyes yet), are likely collagen deposits. It would be easy to check: collagen in mammal skin has a lot of glycine-X-hydroxyproline motifs.32
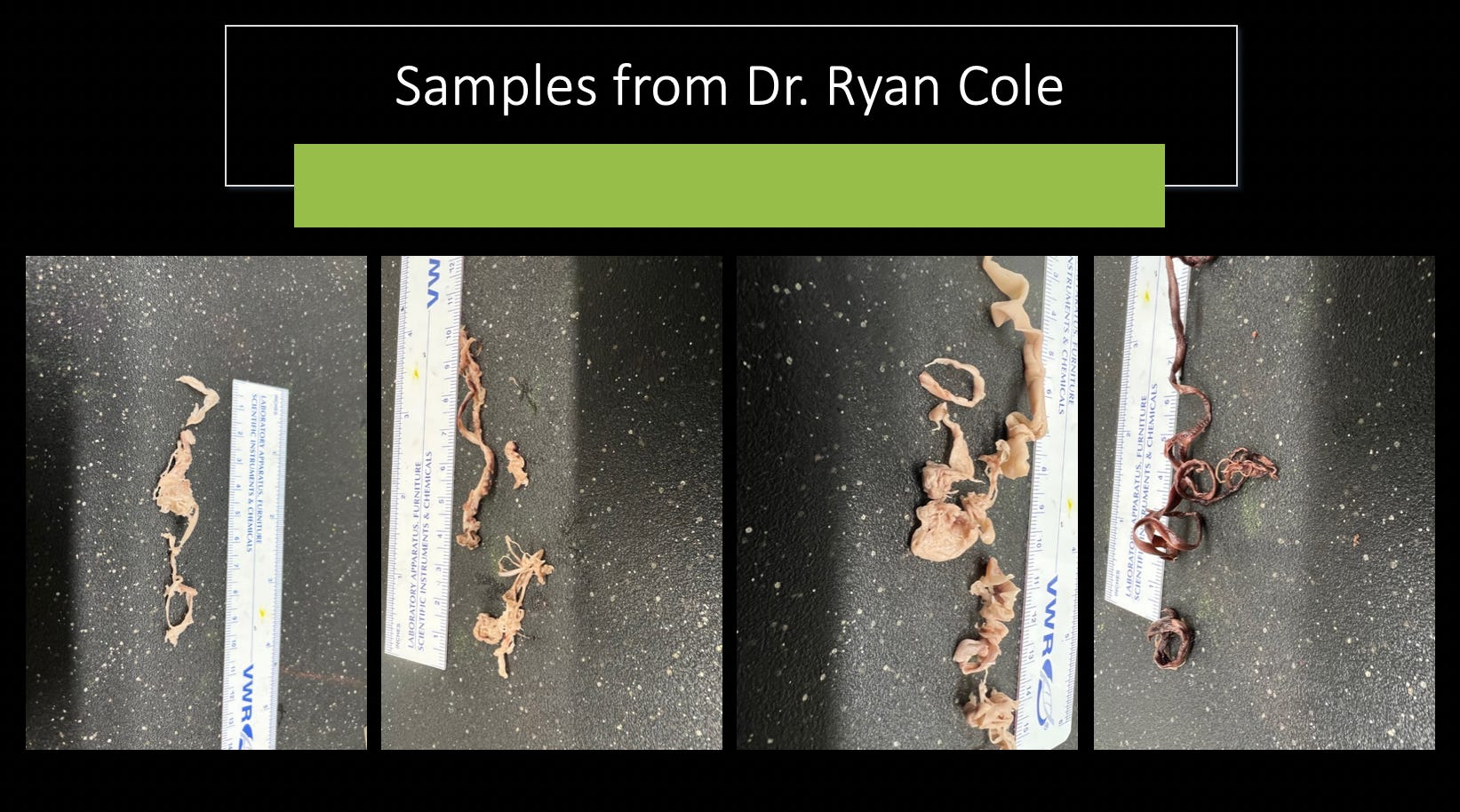
Question: What would happen if Type III collagen deposition in large blood vessels got out control for some reason? How would that manifest? Would it manifest as long, fibrous, collagen-rich obstructions in these vessels? Hmm? I bet my bottom dollar that if those things pulled out of cadavers were compared to any normal collagen-rich materials, they would have close to identical compositions.
Final thoughts: VAERS rustling leaves…
I did a VAERS query for the following listed ‘Uncommon symptoms and complications’ of IgG4RD according to Wikipedia. Just for fun.

There are N = 22,678 reports when querying these exact keywords as a group. The age distribution looks like this when normalized to CDC data:

It looks more damning when you consider the fact that the average number of reports for all vaccines combined for the past 5 years when querying this cluster of adverse events is N = 195, as compared to N = 6111 for the number of domestic reports for the Moderna, Janssen and Pfizer products alone, for 2021. Why are there 31 times more reports of these adverse events in one year for 3 products, as opposed to the past 5 years and at least 64 products? That don’t make no sense.
And just to say I checked, I added the MedDRA code ‘Fibrosis’ to the query and returned N = 23,657 reports for the COVID-19 products.
One more thing on molecular mimicry and Tregs and then I’m done For now. This might actually be good news for people who have enhanced IgG4 serum antibody levels! Or I might be completely wrong. I need to read more on this.
Here’s a paper entitled: “Regulatory T cells and Immune Tolerance”33 where they write:
This might enable natural Tregs to exert dominant and tonic suppression of self-reactive T cells. It could also contribute to the prevention of autoimmunity stemming from molecular mimicry (the antigenic cross-reaction between a self-molecule and a microbial substance) because natural Tregs could be more easily activated than self-reactive T cells by such a substance (Stephens et al., 2005).34
What this means is that it’s possible that if there are more induced Tregs from excessive levels of circulating IgG4 antibodies from the shots, then these Tregs might actually be preventing autoimmunity by over-riding the antibodies that are auto-reactive due to the shots. However, I am not entirely sure since they do make reference to natural Tregs and they might have done that for a reason: perhaps induced Tregs don’t exert these functions as efficiently? Does that make sense?
This article was a lot for me to write up and I am sure, a lot to digest for my readers. So I leave it ‘as is’ for now.
More on the subject of IgG4RD soon. It is gravely important. Pardon the pun.
https://en.wikipedia.org/wiki/Fibrosis
https://en.wikipedia.org/wiki/Connective_tissue
https://en.wikipedia.org/wiki/Collagen
https://en.wikipedia.org/wiki/Type_I_collagen
https://en.wikipedia.org/wiki/Collagen,_type_III,_alpha_1
https://healthmatters.io/understand-blood-test-results/igg-subclass-4
Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. 2014 Oct 20;5:520. doi: 10.3389/fimmu.2014.00520. PMID: 25368619; PMCID: PMC4202688.
https://en.wikipedia.org/wiki/Antigen
https://www.massgeneral.org/medicine/rheumatology/treatments-and-services/igg4
Gutierrez PS, Schultz T, Siqueira SA, de Figueiredo Borges L. Sudden coronary death due to IgG4-related disease. Cardiovasc Pathol. 2013 Nov-Dec;22(6):505-7. doi: 10.1016/j.carpath.2013.05.003. Epub 2013 Jul 2. PMID: 23830124.
Patel NR, Anzalone ML, Buja LM, Elghetany MT. Sudden cardiac death due to coronary artery involvement by IgG4-related disease: a rare, serious complication of a rare disease. Arch Pathol Lab Med. 2014 Jun;138(6):833-6. doi: 10.5858/arpa.2012-0614-CR. PMID: 24878025.
Tsai HC, Tung HY, Liu CW, Su CF, Sun YS, Chen WS, Chen MH, Lai CC, Liao HT, Yang YY, Huang YH, Tsai CY. Significance of high serum IgG4 in complete or non-full-fledged IgG4-related disease-a retrospective investigation of 845 patients and its clinical relevance. Clin Rheumatol. 2022 Jan;41(1):115-122. doi: 10.1007/s10067-021-05772-x. Epub 2021 Aug 29. PMID: 34455508.
Martín-Nares E, Saavedra-González V, Fagundo-Sierra R, Santinelli-Núñez BE, Romero-Maceda T, Calderón-Vasquez K, Hernandez-Molina G. Serum immunoglobulin free light chains and their association with clinical phenotypes, serology and activity in patients with IgG4-related disease. Sci Rep. 2021 Jan 19;11(1):1832. doi: 10.1038/s41598-021-81321-5. Erratum in: Sci Rep. 2021 Jun 1;11(1):11959. PMID: 33469111; PMCID: PMC7815906.
Campochiaro C, Ramirez GA, Bozzolo EP, Lanzillotta M, Berti A, Baldissera E, Dagna L, Praderio L, Scotti R, Tresoldi M, Roveri L, Mariani A, Balzano G, Castoldi R, Doglioni C, Sabbadini MG, Della-Torre E. IgG4-related disease in Italy: clinical features and outcomes of a large cohort of patients. Scand J Rheumatol. 2016;45(2):135-45. doi: 10.3109/03009742.2015.1055796. Epub 2015 Sep 23. PMID: 26398142.
Wallace ZS, Zhang Y, Perugino CA, Naden R, Choi HK, Stone JH; ACR/EULAR IgG4-RD Classification Criteria Committee. Clinical phenotypes of IgG4-related disease: an analysis of two international cross-sectional cohorts. Ann Rheum Dis. 2019 Mar;78(3):406-412. doi: 10.1136/annrheumdis-2018-214603. Epub 2019 Jan 5. PMID: 30612117; PMCID: PMC6996288.
Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Sumida T, Mimori T, Tanaka Y, Tsubota K, Yoshino T, Kawa S, Suzuki R, Takegami T, Tomosugi N, Kurose N, Ishigaki Y, Azumi A, Kojima M, Nakamura S, Inoue D; Research Program for Intractable Disease by Ministry of Health, Labor and Welfare (MHLW) Japan G4 team. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012 Feb;22(1):1-14. doi: 10.1007/s10165-011-0508-6. Epub 2011 Sep 1. PMID: 21881964; PMCID: PMC3278618.
Lin W, Lu S, Chen H, Wu Q, Fei Y, Li M, Zhang X, Tian X, Zheng W, Leng X, Xu D, Wang Q, Shen M, Wang L, Li J, Wu D, Zhao L, Wu C, Yang Y, Peng L, Zhou J, Wang Y, Sha Y, Huang X, Jiao Y, Zeng X, Shi Q, Li P, Zhang S, Hu C, Deng C, Li Y, Zhang S, Liu J, Su J, Hou Y, Jiang Y, You X, Zhang H, Yan L, Zhang W, Zhao Y, Zeng X, Zhang F, Lipsky PE. Clinical characteristics of immunoglobulin G4-related disease: a prospective study of 118 Chinese patients. Rheumatology (Oxford). 2015 Nov;54(11):1982-90. doi: 10.1093/rheumatology/kev203. Epub 2015 Jun 22. PMID: 26106212.
Xia Zhang, Hui Lu, Linyi Peng, Jiaxin Zhou, Mu Wang, Jieqiong Li, Zheng Liu, Wen Zhang, Yan Zhao, Xiaofeng Zeng, Liwei Lu, The role of PD-1/PD-Ls in the pathogenesis of IgG4-related disease, Rheumatology, Volume 61, Issue 2, February 2022, Pages 815–825, https://doi.org/10.1093/rheumatology/keab360
Judith S. Satoguina, Esther Weyand, John Larbi, Achim Hoerauf; T Regulatory-1 Cells Induce IgG4 Production by B Cells: Role of IL-101. J Immunol 15 April 2005; 174 (8): 4718–4726. https://doi.org/10.4049/jimmunol.174.8.4718
Sakaguchi S, Ono M, Setoguchi R, et al. Foxp3+ CD25+ CD4+ natural regulatory T cells in dominant self-tolerance and autoimmune disease. Immunological reviews 2006; 212: 8-27.
Wing JB, Tanaka A, Sakaguchi S. Human FOXP3(+) Regulatory T Cell Heterogeneity and Function in Autoimmunity and Cancer. Immunity 2019; 50(2): 302-16.
https://en.wikipedia.org/wiki/Rituximab
https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02
Zhang, J., Chen, H., Ma, Y. et al. Characterizing IgG4-related disease with 18F-FDG PET/CT: a prospective cohort study. Eur J Nucl Med Mol Imaging 41, 1624–1634 (2014). https://doi.org/10.1007/s00259-014-2729-3.
Stone JR. Aortitis, periaortitis, and retroperitoneal fibrosis, as manifestations of IgG4-related systemic disease. Curr Opin Rheumatol. 2011 Jan;23(1):88-94. doi: 10.1097/BOR.0b013e3283412f7c. PMID: 21037477.
Luke Y.C. Chen, Andre Mattman, Michael A. Seidman, Mollie N. Carruthers. IgG4-related disease: what a hematologist needs to know. Vol. 104 No. 3 (2019): March, 2019 https://doi.org/10.3324/haematol.2018.205526.
Della-Torre E, Lanzillotta M, Doglioni C. Immunology of IgG4-related disease. Clin Exp Immunol. 2015 Aug;181(2):191-206. doi: 10.1111/cei.12641. Epub 2015 Jun 8. PMID: 25865251; PMCID: PMC4516435.
https://www.rarediseasesjournal.com/articles/igg4-related-disease-a-minireview.html
https://rarediseases.info.nih.gov/diseases/6322/ehlers-danlos-syndromes
https://www.worldometers.info/world-population/us-population/
https://rarediseases.info.nih.gov/diseases/2081/hypermobile-ehlers-danlos-syndrome
https://en.wikipedia.org/wiki/Collagen
Shimon Sakaguchi, Tomoyuki Yamaguchi, Takashi Nomura, Masahiro Ono. Regulatory T Cells and Immune Tolerance. Cell. REVIEW| VOLUME 133, ISSUE 5, P775-787, MAY 30, 2008. doi:https://doi.org/10.1016/j.cell.2008.05.009.
Stephens LA, Gray D, Anderton SM. CD4+CD25+ regulatory T cells limit the risk of autoimmune disease arising from T cell receptor crossreactivity. Proc Natl Acad Sci U S A. 2005 Nov 29;102(48):17418-23. doi: 10.1073/pnas.0507454102. Epub 2005 Nov 15. PMID: 16287973; PMCID: PMC1297676.
Gosh! No wonder Luc said most who get jabbed will die in 5 years, and Sucharit said, "If you take these jabs you will go to your doom." And Tenpenny said there are 40 different mechanisms of death in these shots. And Mikovits was shouting warnings too.
Which is worse, having your immune system turn on you or having The WHO, CDC, FDA, FBI, CIA, NIH, DHS, and the RCMP turn against you?