


Dying suddenly in sleep or from a run
The connection to adrenal glands, adrenaline and (perhaps) dysautonomia

Adrenaline is a very powerful vasoconstrictor.
During a stressful situation, adrenaline floods your body within minutes. Air passages dilate, redirecting more oxygen to the muscles to help you fight or run—blood vessels contract to send blood to the heart, lungs, and other major muscle groups.1
Adrenaline is why moms can lift cars and destroy buildings when their kids need protecting - a show of ‘hysterical strength’ - according to some.

Pre-thoughts
COVID-19 injection-induced sudden death during sleep is due to adrenaline surges that occur at night and is perhaps exacerbated by Adrenaline Dysautonomia (AD)2. The adrenaline surge (or rush) results in cardiac arrest due to underlying heart damage. This heart damage is due to scar tissue formed in the myocardium (and pericardium) induced by the immune responses to the foreign proteins lodged there as a result of the shots. A terrible cycle.
I also think sudden deaths might be linked to adrenaline dysautonomia arising due to infiltration of massive quantities of LNPs (and subsequent foreign protein production) in the adrenal glands, perhaps leading to overactive adrenals.3
Two punch knock-out: shot-induced heart scarring and adrenaline
Peter McCullough is an internist and cardiologist who recently spoke on this subject matter in an interview on the Highwire, and about why cardiologists recommend no exercise following a diagnosis of myocarditis. It is because adrenaline surges push the circulatory system to a point where underlying heart damages prevent normal functioning, thus potentially can lead to cardiac arrest. Nobody wants that. So don’t run for a bit.
This is why some people who got the shots are experiencing cardiac arrests during runs. The shots mediate heart scarring via immunological damage and repair/wound healing mechanisms. The scarred heart (scars are the result of wound healing) cannot ‘properly’ endure the pressures imposed by adrenaline surges on the vasculature, ie: systemic vasoconstriction. The heart stops pumping effectively. The heart stops.
These adrenaline surges are normal due to the effects of exercise, for example, but heart scarring is not normal, especially in children, no matter what the CDC says.
You can click on the photo to get to link to a part of his interview.

It seems really clear based on the enormous number of people experiencing heart damage following the COVID-19 injections that these minor heart infractions can ultimately lead to sudden death by cardiac arrest. Any amount of scar tissue in the myocardium is bad, as Peter points out.
But what happens when adrenaline surges happen out of sync with ‘normal surging’ like the kind you experience when you’re exercising?
Dysautonomia and adrenals
Dysautonomia is dysregulation of the involuntary nervous system. It involves the adrenal glands (among other things) which are responsible for producing stress hormones like cortisol, adrenaline and noradrenaline. Think hypothalamic–pituitary–adrenal (HPA) axis when looking at the sympathetic branch. Basically, dysautonomia entails an imbalance of normal hormone production when the autonomic nervous system is not working properly. By the way, amyloidosis is one of the most common causes of dysautonomia, but there are many others including Ehlers-Danlos, HIV and multiple sclerosis.4 My readers already know my theories on cardiac amyloidosis and amyloids in general with regard to the shots. Watch my NCI testimony to learn more or the abridged version by Viva Frei. By the way, he and I will speak again today.

It is also important for me to point out at this point that Postural orthostatic tachycardia syndrome (POTS), also called postural tachycardia syndrome, is a subset of dysautonomia.5
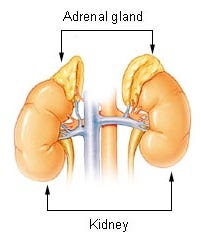
The connection between the shots and the adrenals
As part of bio-distribution and accumulation studies, it was discovered that the LNPs traffic to and accumulate at high concentrations in the adrenal glands. They stopped measuring after 48 hours and it is unknown if the concentrations would have kept increasing.

As everyone knows, the places where the LNPs locate are where they dump their modified mRNA payload. It is therefore not a stretch to imagine that massive amounts of foreign proteins would be produced and expressed in the cells of the adrenals.
So the question becomes, what are the effects of this? Could the adrenals become dysfunctional and produce undesirable adrenaline surges? Could it trigger AD? I can’t think of a reason why some kind of ‘disturbance’ to ‘normal functioning’ wouldn’t ensue. It would be like throwing a bunch of sand into a dough mixture, wouldn’t it? The bread wouldn’t work.
Here are the symptoms of AD:


Sound familiar? In fact, with chest pain, fatigue and breathing problems, one might suspect myocarditis. I would. But it could be both. If you combine off-timing or even on-timing adrenaline surges with heart damage, you get cardiac arrest. I should point out here, based on VAERS data, that only 0.3% of individuals who suffered myocarditis also had signs of adrenal problems. But, this could be a VAERS reporting thing. Just playing my own Devil’s Advocate.
We do not need to consider AD when putting together the cause of sudden deaths for individuals exercising or sleeping. We already know adrenaline surges happen during these times. But imagine if there was AD involvement. The two-punch pathology becomes punchier and not-’chronobiologied’ (I couldn’t think of a better way to put this): scar tissue formation from immune-mediated damage to heart tissue and out-of-step adrenaline surges could cause cardiac arrest at any time. Out of the blue, so-to-say.
What is VAERS saying?
I looked in VAERS for ‘Adrenal insufficiency’, ‘Dysautonomia’, and ‘Autonomic nervous system imbalance’ and ‘Cortisol decreased’ and found 3,332 reports.
Although the number of reports is low when compared to the total number of reports (1,568,559) and the shot administration numbers, when the counts are normalized to shot administration number per age group, it is interesting how the 18-24 age group has the highest frequency of reports per 100,000 doses. And yes, I know. The numbers are tiny. But the pattern is there.

I think it would be very interesting to get some pee and look at hormone levels in post-injection people. I bet tons of people would be up for that. You don’t even need to get injected.
https://www.everlywell.com/blog/sleep-and-stress/cortisol-vs-adrenaline/
https://www.drlamcoaching.com/blog/adrenaline-dysautonomia-known-condition/
This can be checked by measuring hormone levels in the blood and urine.
https://en.wikipedia.org/wiki/Dysautonomia
https://www.drlamcoaching.com/blog/how-a-faulty-sympathetic-response-can-lead-to-afs-and-pots/
A friend in her 80’s who consented to the UK’s “spring booster” keeps fainting. She finally visited the GP, told she has tachycardia and put on beta blockers which are now making her feel unwell. Another friend, in her 80’s, extremely fit, same problem, also drank the most recent koolaid. Funny how the the NHS health professionals keep on ignoring/denying causation. I have witnessed too many coincidences since the start of the administration of covid jabs. So very many people suffering adverse events, many being serious.
How to prevent the people from rising up against you. As most in the western world have poor aerobic strength - when they find themselves whipped into a frenzy, aka a protest, their adrenal glands fire and they have a cardiac arrest. It's a contingency plan to guarantee they retain power for the next generation. Millions of young men, will grow into weaker adults and not have the capacity to fight back against their oppressors.