
A new development in the FOREIGN DATA PURGE missing myocarditis signal story...
To myocarditis be, or not to myocarditis be? That is the question.

First of all, thank you a million times to the brilliant mind of Will Dove of the The Iron Will Report for the spurring this new analysis. Here is a link to a previous interview that we did together.
Thank you also to Liz for your incredible and constant feedback and nerdy data nerd friendship. True collaboration rules.
Will and I were literally in the middle of an interview last night - which has been suspended until next week (December 28, 2022) pending the completion of my new current analysis - where I was re-presenting my live presentation of VAERS data manipulation for the WCH, for Will’s audience. He stopped me at the slide where I present the ‘AFTER’ picture of the loss of the myocarditis dose 3 signal following the VAERS foreign data purge. That slide looks like this:
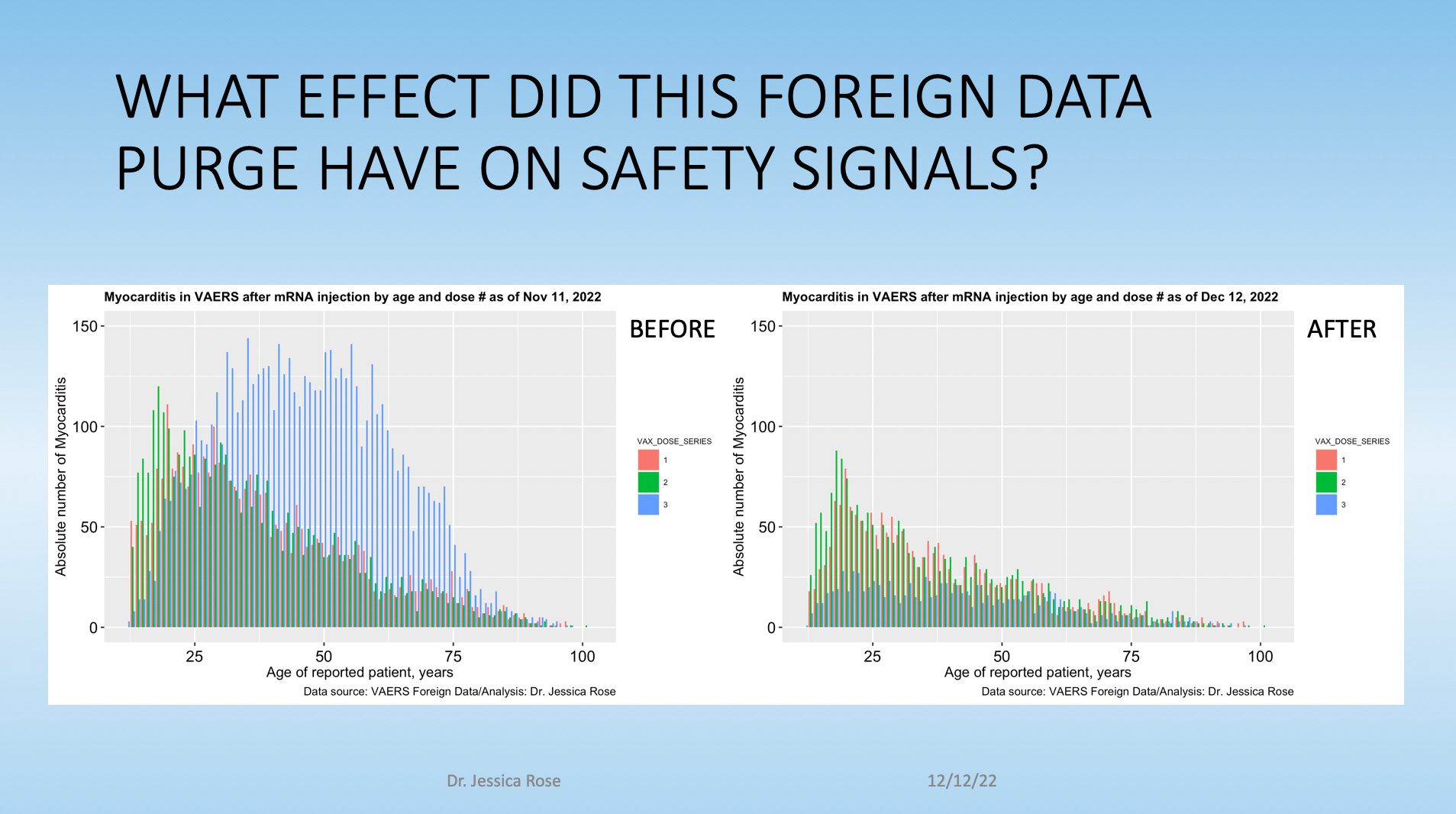
The difference in the myocarditis signal is striking when you compare pre- (Nov 11, 2022) and post (Dec 12, 2022)-data purge. Both the magnitude and the dose 3 response of the myocarditis signal was affected, in extreme ways. In fact, the dose 3 response completely disappeared! Poof! That happened on November the 18th, 2022. Here’s the evidence.

Will stopped me at this slide, as I mentioned, and asked a most beautiful question:
Question: What are the people who once were myocarditis cases classified as now?
I have reported that there were no missing IDs following ‘the purge’; just missing text from the variables that had ‘free text’, so, indeed: What of their ‘case’ status? Just to be very clear about what happened, the individuals - as in, VAERS IDs - did not go missing; the free text in their individual reports did. Free text such as that written in the SYMPTOM_TEXT variable: a variable that contains an enormous amount of information and from which much of the SYMPTOM variables are populated from. This free text went missing under orders from ‘European regulators’ who bitch-slapped the FDA and CDC to remove this free text from these individuals’ variables in the VAERS foreign data file.
At the time when I found this and reported on it, mentally, I had stopped at “they are no longer myocarditis cases”, and I didn’t go any further. I reported on it in Unacceptable Jessica here and here, did some presentations and then moved on to other things. I have been speaking extensively about the lost myocarditis dose 3 response. But this is an incredible follow-up piece! And I need to follow-up! So, Will and I decided to stop (recording) the interview, and to reschedule for a week from yesterday. Stay tuned! (I will post the interview here, promise.) And then I went to work. P.S. Thank you Will. This is how it’s done.
P.P.S. Me and Liz were talking all morning about this issue and, as usual, our collaborative efforts ended up being a smorgasbord of synergistic mutual benefit. I raise a glass of wine (or 3) to Liz, and Will, and all of you, and to friendship and collaboration! Down with division. Here’s the real raw truth from the real raw data.
It’s PROOF. Use it. Don’t abuse it.
Boring (but important) stuff first
When doing keyword searches for myocarditis cases, I ask R to ‘look through’ the SYMPTOM columns and the SYMPTOM_TEXT column for the word ‘Myocarditis’ or ‘myocarditis’. I do this since I am worried that ‘they’ might try to hide a myocarditis case in the SYMPTOM_TEXT column. Makes sense, right? Here’s a demo of a list of VAERS IDs with the SYMPTOM variables and the SYMPTOM_TEXT variable, albeit truncated for ease of demo.

One thing that is very important to bear in mind when analyzing VAERS data is to know ahead of time if you are seeking adverse event report counts, or counts of reports per individual. I always count reports of individuals. You’ll notice in this demo screenshot that VAERS ID 945726 has two columns taking up space with a total of 7 reported MedDRA codes. I’ll return to this. For now, here are some basic statistics on the difference between the data sets for November 11, 2022 and December 12, 2022.

Instead of showing you tables of numbers of adverse events that, in effect, wouldn’t be different between the pre- and post-purge data sets to answer the question: “What of their ‘case’ status?”, what I decided would be the most useful thing to show you guys here is definitive proof of data manipulation in VAERS by specific examples, and how this purge really is theft of safety signals.
Think of two scenarios that would make you go: ‘hmm’. No, seriously. Think about it. Imagine the text fields were gutted and then write down what the most relevant questions to you would be. No seriously, write them in the comments.
Got them? Here were mine.
Are there cases of myocarditis that were (prior to purge) in the SYMPTOM_TEXT variable that do show up as MedDRA codes in the SYMPTOM columns? This would indicate a non-loss of signal for those individuals.
Are there cases of myocarditis that were (prior to purge) in the SYMPTOM_TEXT variable that do not show up as MedDRA codes in the SYMPTOM columns? This would indicate a loss of signal for those individuals.
Answers: Yes and Yes.
By the way, I am working on a descriptive statistics analysis so you guys know what percentage of cases qualify as 1 or 2.
Before I present the cases, I want to make a point about the importance and relevance of the SYMPTOM_TEXT variable. Let’s look at the individual with VAERS_ID 945726. This particular individual did not have their SYMPTOM_TEXT deleted but the text is a good example of how much information can be present in this field.


For my dear poorly-visioned readers (like myself), here is a numbered list of what the red highlighted text reads with snarky obvious points in italics that follow:
“Twenty-four hours after receiving the vaccine, he arrived at the emergency room.” (Ahem: temporality → causation - no one would argue that if this person had suffered an anaphylactic reaction in this timeframe that it was not caused by something in the injection)
“Released on diagnosis of viral illness.” (Viral, eh? Are we talkin’ SARS-nCoV-2 viral?)
“Myocarditis” (See “Myocarditis”.)
“There could be a connection to the vaccination.” (Reeeeheeeeeeheeeeeheeeellllyyyyy. This is admission/testimony of the clinician/attending who filed this report, in my opinion.)
“The guy came to us with low blood pressure and was in danger in death.” (Death, eh? That sounds serious.)
“Care should be taken in the vaccination of people who have previously had corona.” (Really? You don’t say. It’s almost as if it makes sense to do serological testing prior to injection, as par for the course, and also to provide instant exemptions from having to be forced to take this crap if antibodies are already found to be present from the individual having experienced natural infection.)
“His condition is currently defined as mild after he was hospitalized in intensive care.” (Mild? He almost died according to the attending! See point 5.)
“Here around 2 million doses of Pfizer’s vaccine have been given and this is the first severe and life-threatening case that has been discovered.” (The first, eh. Wow. That doesn’t match the fact that 24% of VAERS reports currently qualify as severe.)
“The outcome of the event is unknown.” (No follow-up.)
Apparently, according to the reporter, this was the first severe adverse event case report ever! This person is beyond unaware of the current situation with regard to severe adverse event reports in VAERS, and in reality, I dare say. Maybe from his point of view in his clinic, he hasn’t seen many people almost die in temporal proximity to getting these injections, but according to VAERS, this is not the exception - it’s more like the rule. Again, currently (as of December 16, 2022) in VAERS, severe adverse events are at 24% of the total - 9% above normal according to VAERS handbook.1
On the cases
Case 1:
VAERS_ID: 1856190
Shown in Table 2 are the adverse event reports (as MedDRA codes) submitted for a single individual assigned VAERS_ID number: 1856190. This individual has a total of 10 adverse events associated with their experience with the COVID-19 injections.2
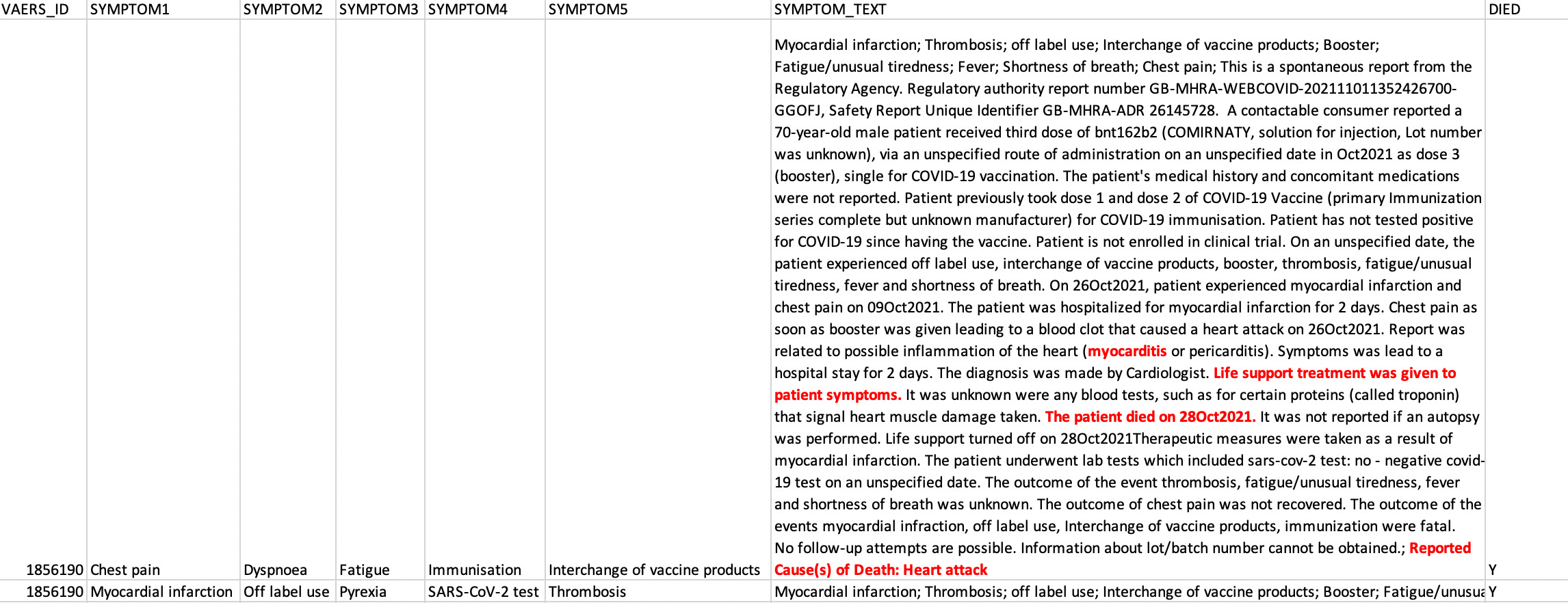
Notice the lack of Myocarditis as a MedDRA code in the SYMPTOM variables? We see Chest pain, Dyspnoea, Fatigue, Immunisation, Interchange of vaccine products, Myocardial infarction, Off label use, Pyrexia, SARS-CoV-2 test, Thrombosis. No Myocarditis. This individual did, in fact, clearly have myocarditis reported in the context of their VAERS report (highlighted in red in Table 3 below) reported in the SYMPTOM_TEXT field.
The SYMPTOM_TEXT field for this person with VAERS_ID 1856190 in Table 3 is an essay. And it is FULL of information. It was deleted. Wah-pah!
Prior to the deletion of the SYMPTOM_TEXT field data for this individual, there was no addition of the myocarditis report to any of the SYMPTOM variables. Was it was too difficult to add a Myocarditis MedDRA code to one of the SYMPTOM variable fields in this individual’s VAERS report?
What might be even more shocking here is the report of this individual’s death that was also not translated to the SYMPTOM columns as a MedDRA code.
So to refresh ourselves on how shocking this is, this individual, who remains in the foreign data set with their VAERS_ID intact, who had someone go to the extensive trouble to file this VAERS report, had their free text fields eviscerated by ‘European regulators’ - but before that happened, there was no cross-check of adverse event reports in the SYMPTOM_TEXT to MedDRA codes in the SYMPTOM variables. The only thing I can think of that would be a reasonable non-nefarious reason for doing this, is if a keyword search was done using the medDRA code ‘Myocarditis’ in the SYMPTOM_TEXT column, and it was missed due to the lack of capitalization of the word. But given that ‘Death’ is, in fact, written as a MedDRA code in the SYMPTOM_TEXT field and also not transferred to the SYMPTOM variables, I smell a rat. Either a lazy rat, or very naughty rat.
The effect of this is that this individual’s myocarditis (and death) case no longer gets counted. Signal → lost.
That’s the best-case terrible scenario from an ‘intention’ point of view. In the worst case scenario, someone actually did notice ‘myocarditis’ in the SYMPTOM_TEXT field, and just didn’t bother to add it to the MedDRA code list as a SYMPTOM which would, in effect, [intentionally] eliminate that individual’s myocarditis signal from this data set. I tend to think the former scenario is the likely one: there simply are not enough qualified people to handle this amount of data - even with their new hires.
This is perhaps one of the most important points I can make here: the fact that the owners of this amazing and huge data set are not doing everything possible to ensure that this can be the best pharmacovigilance data set it can be, is malfeasant. The fact that they are not representing the date as it is reported, is fraud. They are not only not making it all it can be, they are pretty much ignoring all of the safety signals (not just the myocarditis signals) and thus, THE PEOPLE, who have been injured and managed to report their injuries, therein.
Either way, this is data manipulation. Question: Is it not fraud to misrepresent a government data set like this? I mean, it’s written on the VAERS website very clearly that to file a false VAERS report is a felony, so wouldn’t fudging the data also be? And geez, most importantly, what of this 23-year-old man? Did he survive? We will probably never know, because: no follow-up.
This individual deserves better than this, and trust me when I say this: This is your data too. It’s your loved ones’ data. Lost time. Lost lives. Preventable tragedies. Real experiences. That all matter.
I dare say that this is certainly NOT what anyone signed up for when they got injected.
Case 2:
VAERS_ID: 961992
This case is also pretty precious. This individual still counts as a myocarditis case even after having their SYMPTOM_TEXT deleted. As shown in SYMPTOM2 in the second row of their adverse event report, myocarditis is clearly marked by the MedDRA code “Myocarditis”.

N.B.: When counting VAERS IDs, one does not count reports of adverse events; one counts the IDs. One may remove duplicate VAERS IDs, as one should - so as not to over-count the VAERS IDs. The second row (or the third, if it exists) of the SYMPTOM data should be ‘spread’ to include additional columns of adverse event data as per VAERS ID. I am showing it this way (as per Table 4) because it would look way too ugly to spread the SYMPTOM columns over 10 variables.
Myocarditis appears as the 7th MedDRA code (in the 2nd row under SYMPTOM2) after ‘Lipids’ (what the hell?). Did you happen to notice what the first entry in the first row is? COVID-19. That’s right. Oh man, this guy’s definitely gots da COVIDs. Gotta be. Everyone’s got it right? This person got COVID and that’s why they’re messed up. It’s not because of the injection they got a few hours before. *Sarcasm detector about to implode.
But wait. There’s more. Did you notice what is written in the SYMPTOM_TEXT field? “SARS-CoV-2 infection”. So this guy had SARS but not COVID? When?
Here’s his SYMPTOM_TEXT for you to read.

But wait. There’s more. Did you notice what is written in the HISTORY field? “Patient has not had symptoms associated with COVID-19.” Wait, what? Then, how. What? Wait. Could this be one of those false positive PCR ‘tests’ showing someone as being ‘positive’ for ‘SARS-nCoV-2’ when, in fact, they did not have SARS-nCoV-2 or COVID? Well, yes, they certainly do report a ‘positive’ COVID swab in this person 5 days following his second injection, but that’s not worth much. Combine the incredibly high false positive rate of the PCR ‘test’ due to the use of ridiculously high cutoffs, and the fact that this guy had no COVID symptoms, COVID-19 should have been ruled out, not in. The verdict should have come down to serology but serology was not done for this particular individual. The attending physician reported that he had myocarditis. Maybe he had myocarditis? I just don’t believe this is what we get. And these people are calling it ‘science’.
Let’s re-cap. He didn’t have COVID symptoms at the time of hospitalization. But he was hospitalized. And lo and behold, ‘PCR’ed. Since the PCR ‘test’ came back ‘positive’, they can say he had COVID! But, in reality, he, also… had myocarditis? Onset right after the injection. So yeah, let’s call it COVID. Great. Everything’s COVID. COVID. COVID. COVID. Even though myocarditis did make it to MedDRA coding, so did COVID-19. It is my opinion that it should not have.
These 2 cases are anecdotal by themselves. I know that. But I wanted to get this message out as clearly as I could, hence why I chose 2 specific examples. I want you guys to spread this evidence around. It IS evidence.
In Case 1, we had SYMPTOM_TEXT deleted, and the myocarditis signal was lost because it was not filled in as a MedDRA code in a SYMPTOM field.
In Case 2, we had SYMPTOM_TEXT removed, and the myocarditis signal was not lost because it was filled in as a MedDRA code in a SYMPTOM field.
These inconsistencies are very bad.
I am in the process of doing a complete analysis on ‘THE_LEFT_BEHIND” data set, and will update ASAP. It is going to take some time, as I am literally doing 10 million things at once.
I plan to characterize the individuals who had their data gutted. I will leave you with the following. It is a very simplified bar plot showing cardiac-associated adverse event reports extracted from SYMPTOM1 in row 1, only. I did this on purpose just to present an idea of the spread of the cardiac-associated adverse events for these people.
The x-axis is a little cluttered but what this very blasé chart shows are 280 MedDRA codes related to cardiac ‘issues’ and the number of reports for each. I also included some vascular-related injury codes. These MedDRA codes likely belong together as sub-symptoms or tests pertaining to myocarditis. These cardiac issues, when clustered, comprise 9.8% of all the reports for THE_LEFT_BEHIND. Thus, I know for now, that ~10% of these left be-hinders did suffer cardiac issues - just definitely not myocarditis. By the way, this is a ‘technique’ used to hide signals in data: distribute the signals over a wide range by calling them all sorts of different names.

But a rose by any other name would smell as sweet.
More soon.
https://vaers.hhs.gov/docs/VAERSDataUseGuide_November2020.pdf
They are actually written in alphabetical order and this is going to be my next Substack.
Is it true that the Warren Commission is now investigating the missing VAERS data?
Another Home Run from our favorite Safety-Signal-Sleuthing-Surfer!!
Thanks for all you do. Best
To FluRona.