
Surgisphere 2.0 - the new JAMA study that says the COVID shots are cardioprotective
Good controls and RCTs be damned!

A new study is being pumped into the world of scientific paper-land entitled “2024-2025 COVID-19 Vaccine and Major Adverse Cardiovascular Events Among US Veterans”. The claim of the authors of this study is the following:
Receipt of the 2024-2025 COVID-19 vaccine was associated with reduced COVID-19–associated cardiovascular risk; evidence of vaccine effectiveness against the broader outcome (all-cause major adverse cardiovascular event (MACE)) likely reflects the hidden burden of undetected SARS-CoV-2 and associated complications that are amenable to reduction by COVID-19 vaccination.
Here are my simple answers to questions for a new article coming out in The Defender. They will help to clarify why the claim is unfounded. I mean, you know, besides the obvious reasons why.
What are the main problems with this study from a methodological perspective (if any)?
It’s an observational study, not an RCT - baseline comparability is everything. Their survival curves show all-cause mortality separating by ~day 10, MACE separating by ~week 5 and all-cause death by ~week 2 which is implausibly fast for a true vaccine effect on these outcomes. The only realistic explanation is that the “no vaccine” group might have sicker/frailer from the start.
What are the main problems with this study in terms of the results – in relation to cardiovascular conditions – and how they were interpreted and presented (if any)?
See above answer. Bad controls/falsification tests: All-cause mortality is a good one here because a vaccine shouldn’t rapidly cut deaths from all causes if the groups are balanced. Quick separation screams confounding.
What are the main problems with this study in terms of the results – in relation to overall vaccine benefits and the cohorts where these benefits were noted – and how they were interpreted and presented (if any)?
See above answer. This is Surgisphere 2.0. This paper should not have passed peer-review.
What are the main problems with this study in terms of the results it presents among the vaccinated vs. unvaccinated cohorts (if any)?
The study design tried to mitigate healthy vaccinee bias via flu-shot-only controls and weighting but failed, as proven by the supplement’s time-to-event curves. This invalidates causal claims about the booster’s cardioprotective effects. The results largely reflect who chooses extra vaccines rather than vaccine efficacy itself. Randomized or better-controlled evidence is needed.
Please share your thoughts on Prasad’s analysis – what would you add to it, if anything?
Prasad is right.
What do the study’s results and data actually tell us?
Nothing. Because the study design is flawed and cannot support causal claims. The study’s data show very small absolute associations between the 2024-2025 COVID booster (in flu-vaccinated veterans) and lower cardiovascular risks. It was allowed to pass peer-review to pump out a false narrative, in my opinion.
Is there anything else you would like to add, not covered by the above?
No. I think I covered it.
Jess
In a nutshell, everyone in this study got a normal old-school flu shot. One group also got the new mRNA COVID shot on the same day. The other group (control) got only the normal flu shot. The claim is that getting the COVID shot with the flu shot that day gives a little extra protection against heart problems. But again, this study is flawed and therefore the claim is baseless because the ‘flu-shot-only’ group could have been full of people who were sicker, frailer, or less healthy overall, so they naturally had more heart problems. It wasn’t a fair comparison.
Not only that but it was a very low-risk period for COVID (lots of prior immunity, milder variants). That’s why the heart problems were extremely rare anyway (only ~2 extra events per 10,000 people in 8 months). If they looked longer (ie: 1–2 years), the tiny “benefit” might disappear or even reverse.
Basically, I can put it to you this way. If me or any of my colleagues had used the methodology designed in this study in an attempt to prove causation between myocarditis and the COVID-19 shots, we never would have been published because the reviewers or editor of whatever journal we might have selected to submit to, would have rejected the study for the reasons listed above.
You can’t have it both ways. Do you see my point?
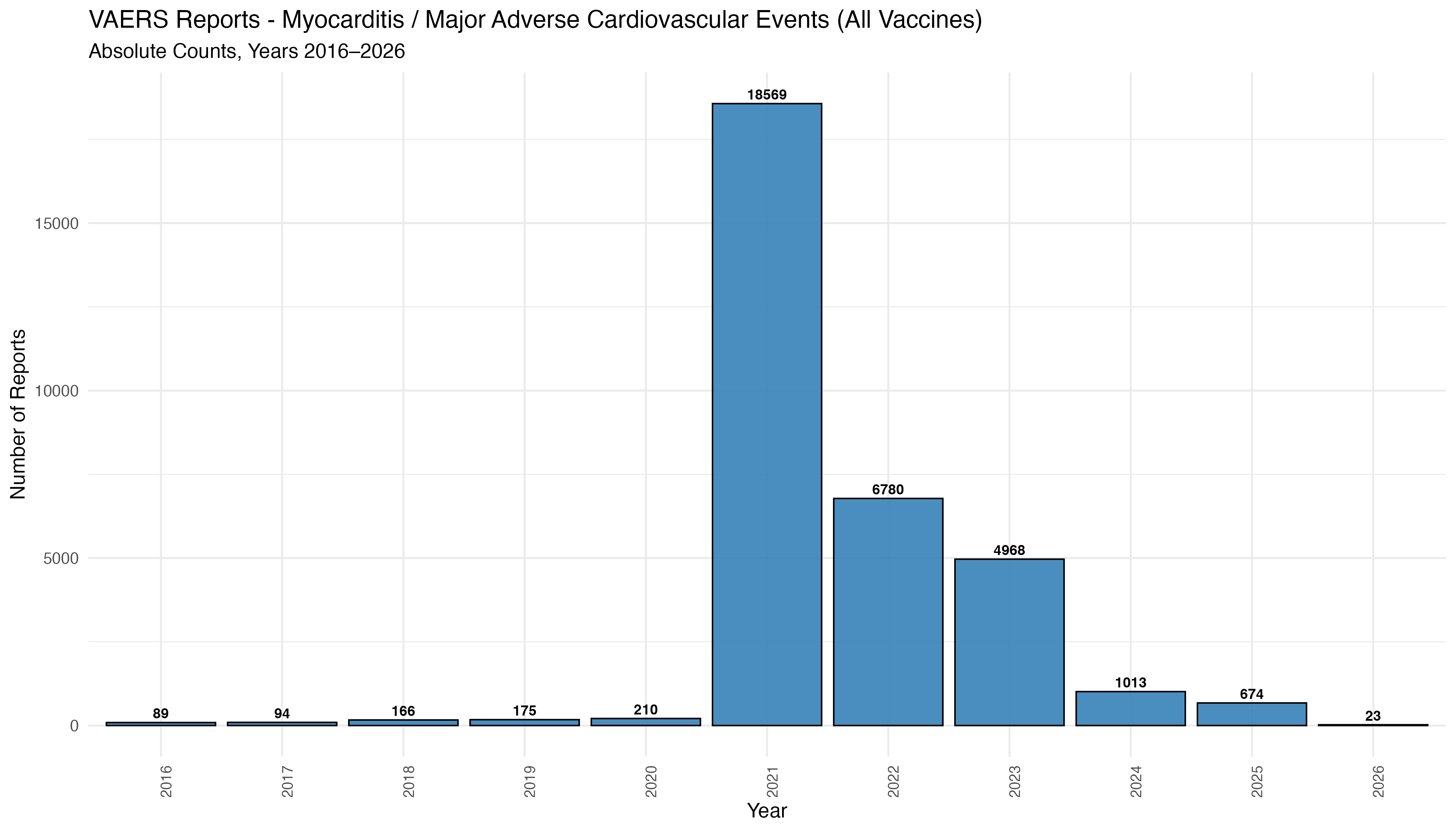
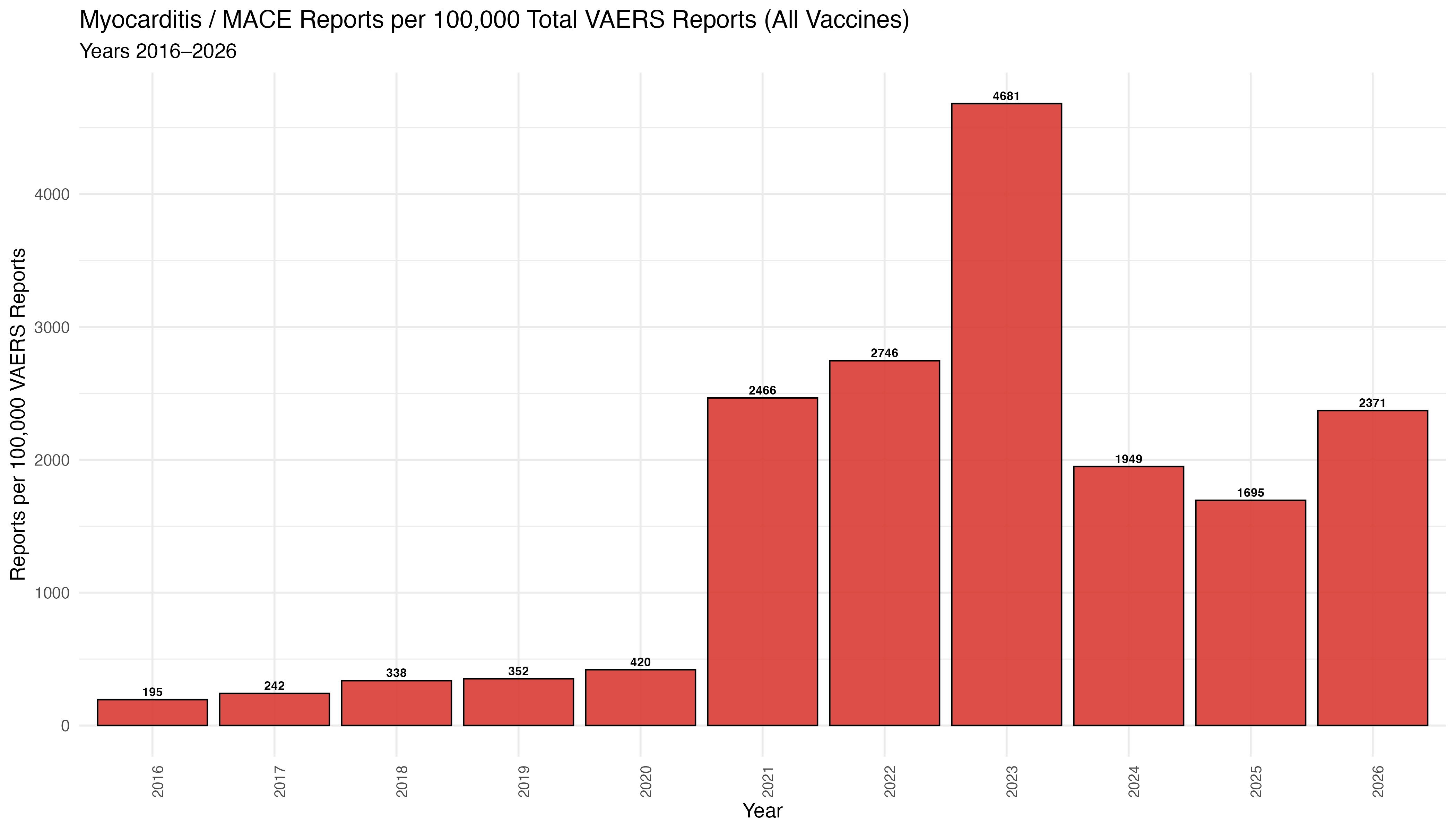
And by the way, the myocarditis/major adverse cardiovascular events (MACE) signal in VAERS is alive and kicking as of 2021. I would suggest the authors of the JAMA study look at the actual adverse events reported to pharmacovigilance databases like VAERS, and then redo their study using a decent control group.
Le conclusion
The methods in this study are snazzy, and the all-cause MACE, etc. reductions appear larger (suggesting benefits against undetected infections), but this study is crap so appearances don’t matter. Healthy-user bias or unmeasured confounding (ie: health-seeking behavior, frailty, or access) are issues. The control group is not a control group - it should have comprised people who were exactly the same as in the COVID shot group → same age, same health problems, same willingness to get vaccines - but who got a placebo (actual saline) instead of the real COVID mRNA shot on the same day as their flu shot. That way, everyone still gets the flu shot where the only difference is the real COVID shot vs saline shot. No “refusers vs. eager people” problem.
This is what a real randomized placebo-controlled trial would have looked like.
Also, the extremely low event rates reflect a low-risk period with hybrid immunity and/or milder variants, and the outcomes rely on ICD codes tied to COVID diagnoses which obviously risks under-ascertainment or misclassification.
I think the reason this paper was written and published is because it was meant to provide “reassuring real-world evidence of incremental benefit” (in the context of the high-risk elderly). But in any case, it overstates certainty for broad policy given the narrow absolute gains and design constraints. I would go as far to say that this paper was published in order to quell people’s concerns about the nucleoside modified RNA-LNP platform because of the plan to usher in the age of all “vaccines” being built using this tech.
Think about it. If people linked the tech to injury - as they should be doing and would be doing if not for censorship and propping up studies that shouldn’t make it past peer review - they would never accept this tech again, in any context.
And then, horror of horrors, the stock prices would crash.
So, does adding the COVID shot on the same day as the flu shot give extra protection against heart problems caused by COVID? No sir. No it doesn’t. Not even if JAMA says it does. Not even if they actually did a proper RCT. In fact, if they did do a proper RCT where they looked past 8 months, my bet would be that they’d see a hell of a lot more MACE, etc. in the COVID shot arm. But we’ll never know, will we?
Surgisphere me once, shame on you.
Surgisphere me twice, shame on me.