

The Bradford Hill Criteria - 'cuz the cowards of Causation denial need complete conversion
The Bradford Hill Criteria - 'cuz the cowards of Causation denial need complete conversion
Slide by slide - all criteria assessed.

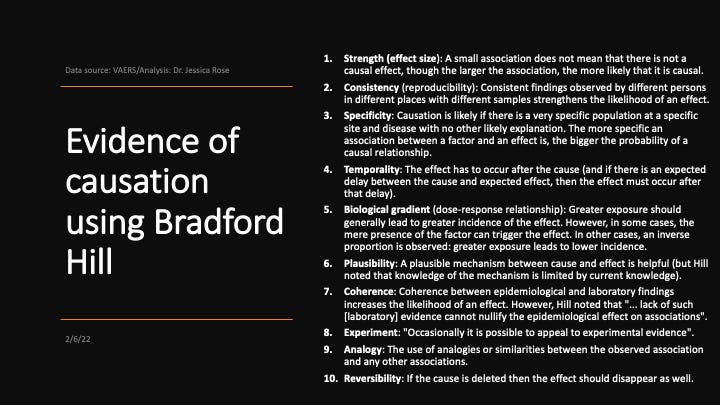
Slide 1: The 10 Bradford Hill Criteria. The World Health Organization (WHO) requires that only 5 are satisfied to show evidence of causation. I will use 10.
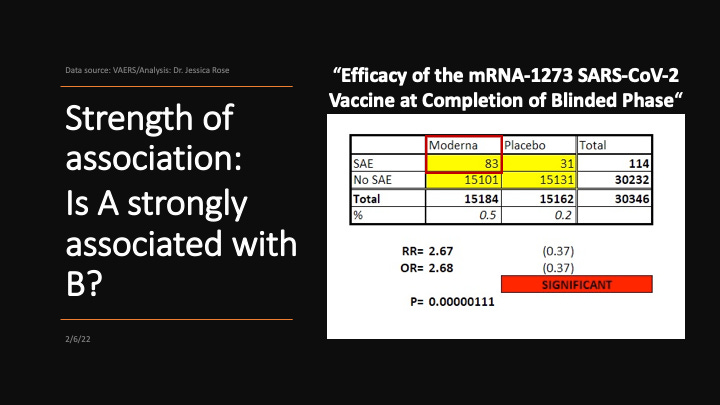
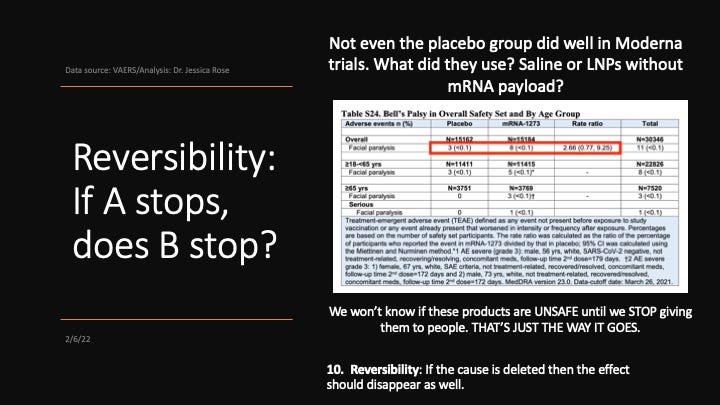
Slide 2: This is Moderna’s ‘efficacy data’ that reveals safety issues. The chi-square test indicates a statistically-significant difference between Severe Adverse Events (SAEs) in placebo versus messenger RNA (mRNA)-1273 groups. And it’s messed up how 2.7 times higher rate for mRNA arm. Sounds like old Moderna needs to go back to the drawing board to me.
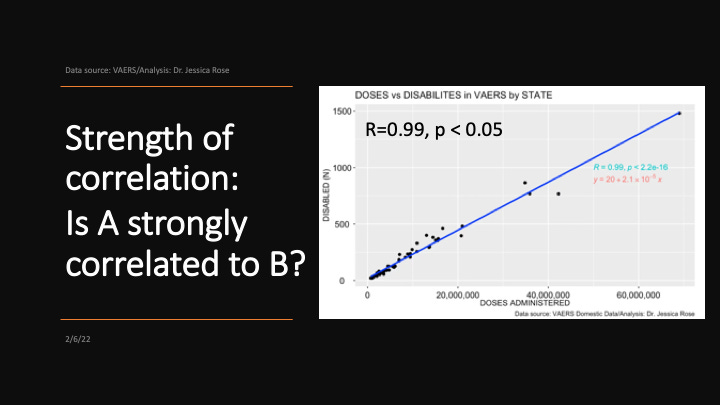
Slide 3: R = 1 means perfect correlation. Not by chance. Each dot is the number of doses/disability per state. Thanks to the mouse.
Slide 4: Same but different.
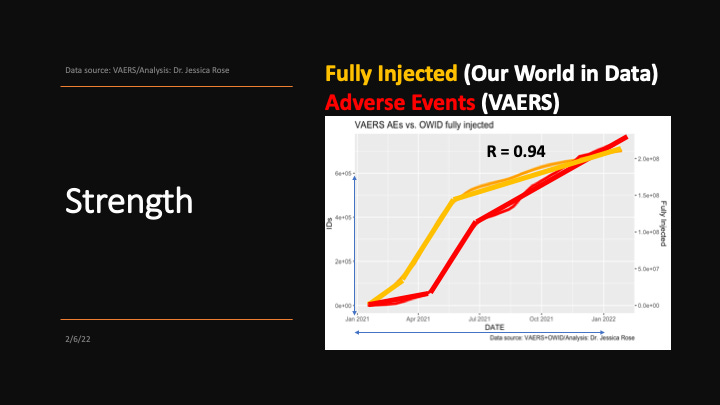
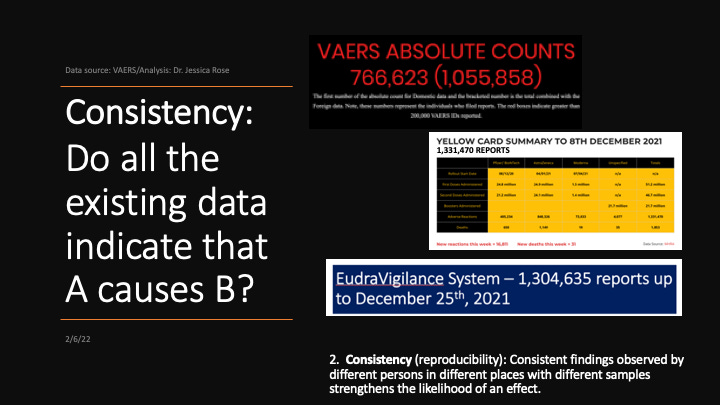
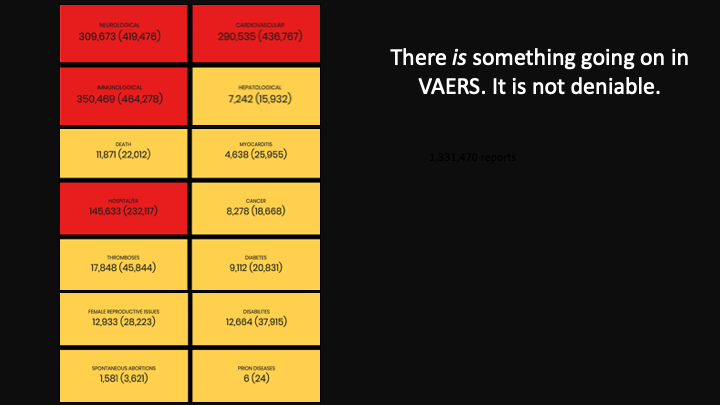
Slide 5: The 3 biggest adverse event data collection systems are showing the same thing: over a million adverse event reports in the context of the COVID-19 injectable products never before seen. They are independent systems.
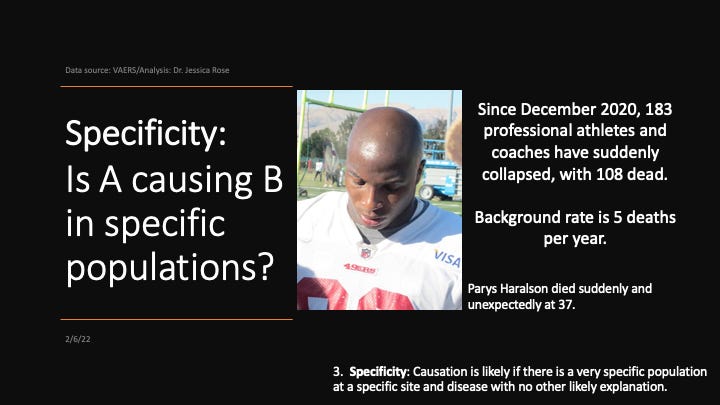
Slide 6: Healthy young athletes suddenly dying from heart failure.
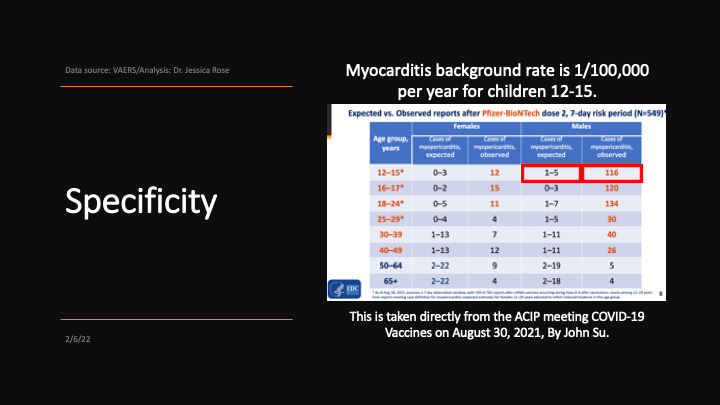
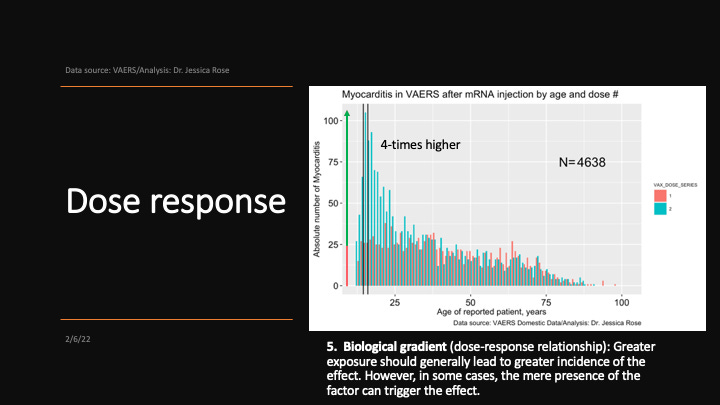
Slide 7: Healthy young children suddenly developing debilitating myocarditis.
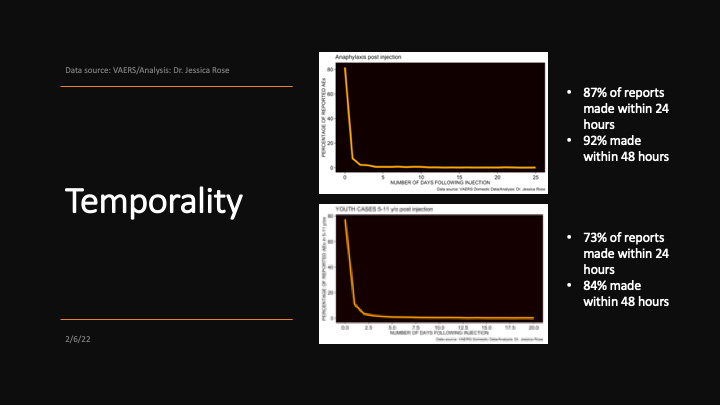
Slide 8: Anaphylaxis is an internal control - an acute reaction to a trigger of which 92% of reports make it into VAERS. Almost the same for kids 5-11 years of age. Temporal gap between injection dates and onset dates narrow @ < 48 hours.
Slide 9: There is 4 times the reporting frequency for 15 year olds following Dose 2.
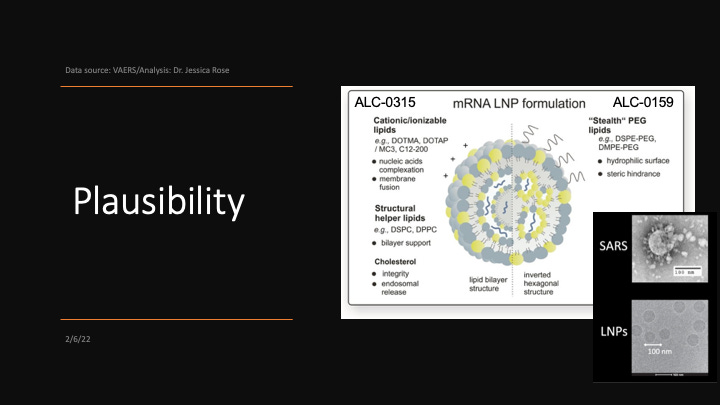
Slide 10: There are 2 mechanisms of action through which I can imagine that these products are wreaking havoc on human physiology: the Lipid Nano Particles (LNPs) and the modified spike protein.

Slide 11: LNPs are toxic on their own - cationic lipids are not pleasant for cell membranes. At all. Neither is PolyEthylene Glycol (PEG).
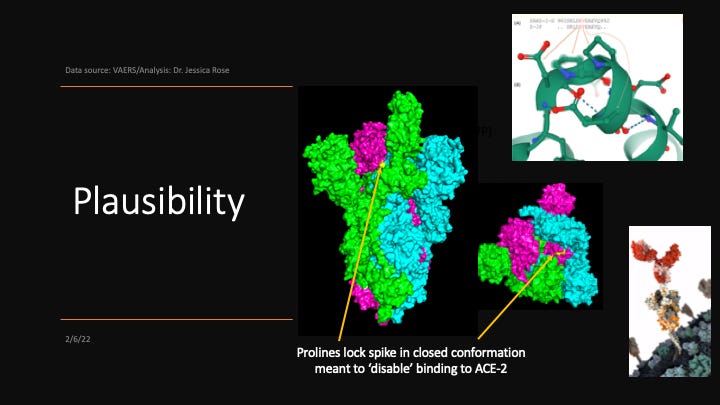
Slide 12: The spike protein of virus is not the same as the modified spike encoded by the mRNA packaged in the LNPs.

Slide 13: There are 2 proline substitutions to ensure closed conformation of spike and ‘unbindability’ to ACE-2. At least, that was the idea. I believe that it can still bind to induce downstream signalling events via ACE-2. All uridines (nucleosides) in the mRNA strand were replaced with pseudouridines (isomers of uridines) to evade Toll-like Receptor (TLR)/innate system detection.
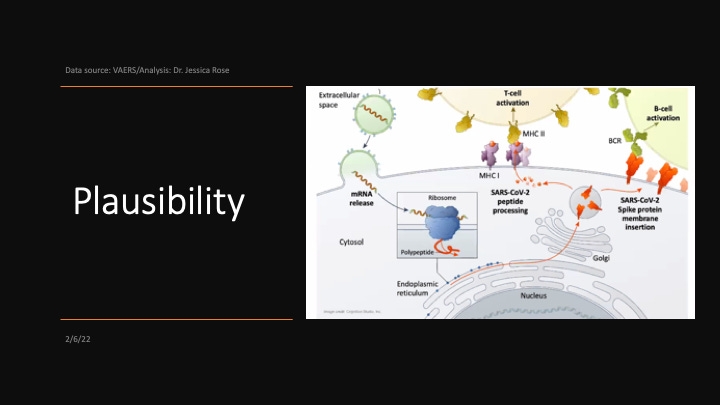
Slide 14: The processed spike bits (antigenic epitopes) are mounted on MHC-class-I and II molecules for CD8+ and CD4+ T cell recognition, respectively, and also B cell recognition by impregnated spike. Cells manufacturing modified spike proteins showing these ‘flags’ are marked for destruction.
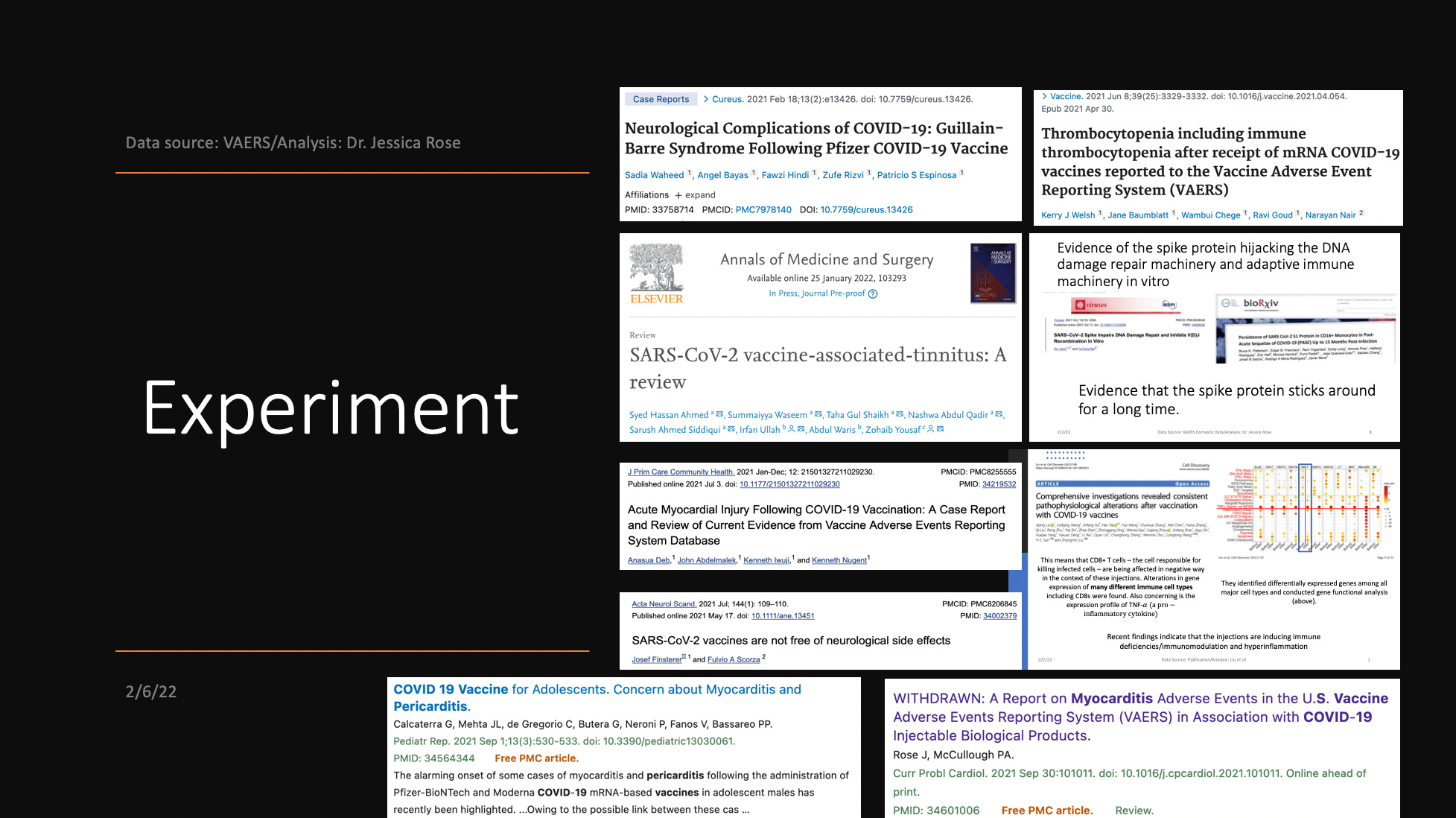
Slide 15: Papers.
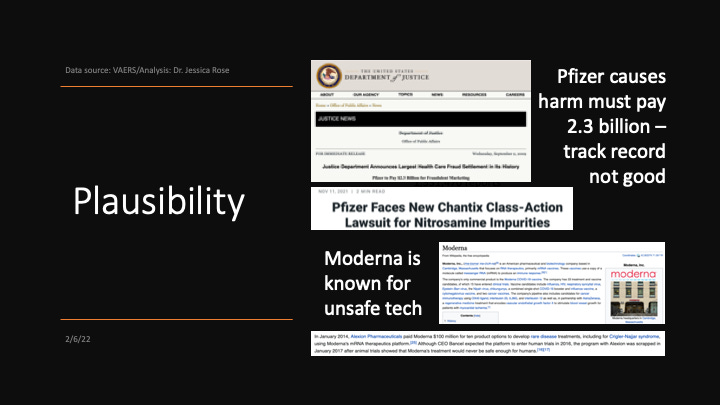
Slide 16: Bad track records.
Slide 17: Moderna ‘efficacy’ data versus what we see in VAERS.
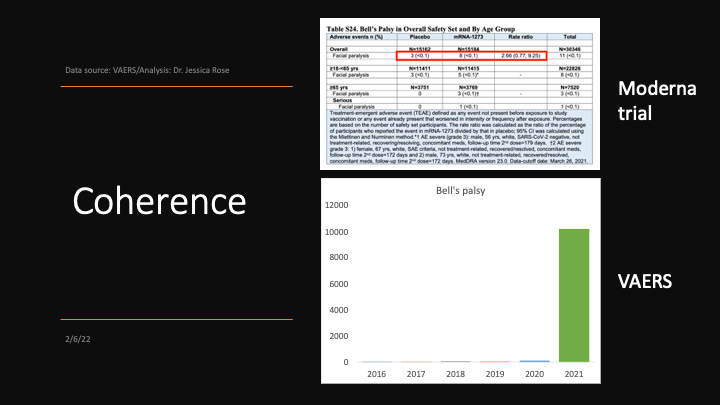
Slide 18: You can choose any adverse event from VAERS. There are currently 10,910 different MedDRA codes (adverse event types) in the VAERS Domestic data set alone. I chose Bell’s palsy as an example.
Slide 19: Papers/case studies.

Slide 20: This roll-out isn’t a Randomized Controlled Trial (RCT) per se, but it is an experiment set for completion in 2023. The adverse event data collected is vital. After all, ‘we won’t know how safe these products are until we put them into people’. Right Rubin?
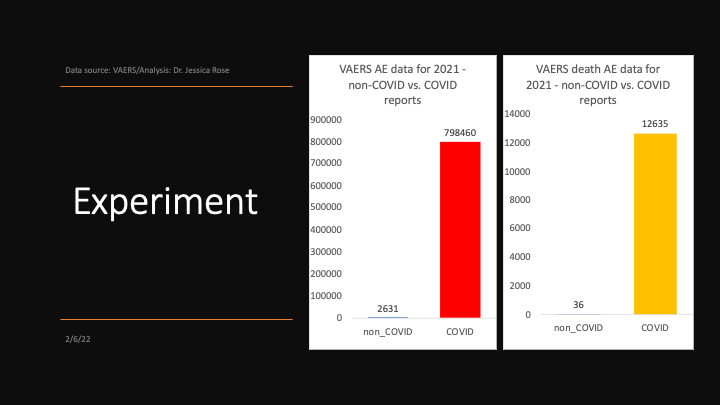
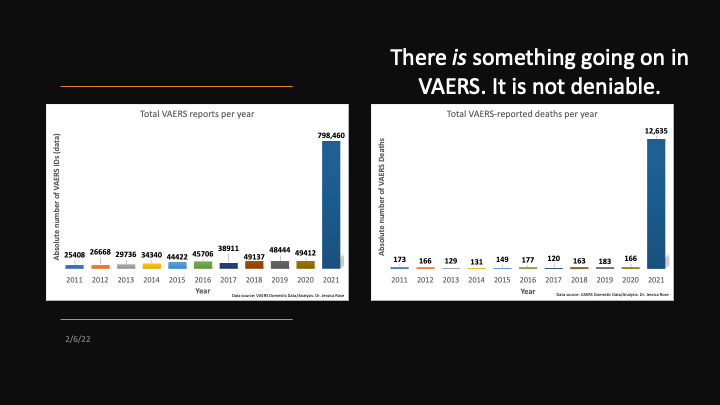
Slide 21: Adverse event data (left) and death data (right) in the context of the COVID-19 injectable products from VAERS Domestic data compared with all adverse event data collected for all other vaccines combined for 2021. There were hundreds of millions of doses of other vaccines administered in 2021, by the way.
Slide 22: A few Papers.
Slide 23: There are many examples: I chose Intussusception because I like the word Intussusception.
Slide 24: Reversibility won’t be possible to show since the adverse event reports will keep coming in even when/if the roll-out slows down/stops. I think these injections are causing immune deficiencies (in some people). I really want to find out in whom.
Slide 25: Problem.
Slide 26: Q?
Slide 27: In your face non-deniability.
Slide 28: And again.
Slide 29: Have at it WHO. Cowards.

Slide 30: Thank you.
MIC. FREAKING. DROP. 🎤👏
Brilliant! Thank you for sharing your presentation slides on Bradford Hill. Will be developing a graduate-level epi and evidence-based practice course soon. I plan to use your work - with proper acknowledgement to you, of course, unless you object - to teach the Bradford Hill Criteria in an authentic way. This will also drive home the message to the nurse practitioner students (NP) about "assuming" vaccines are safe because the "experts" have said so. As a retired NP/educator, I was so naive about this until recently. Thank God for your work and that of Malone, Kennedy, Berenson and the many other true scientists who have taken the time to do the detective work and spoken out. You rock!