


Starting on January 12, 2021 at 1:51 pm ...
Safety signals were clear and weekly updates were being provided...

Again, thank you to ICAN and Aaron et al for getting these documents to the public. Head here.
This document includes all VAERS Meddra coded Preferred Terms with data mining alerts (i.e., EB05 >2) for all EUA SARS-CoV-2 injectable product VAERS reports from weekly ‘US Signals Summary Table’. It includes weekly updates from January 10, 2021 up to and including July 1, 2022.
For download:
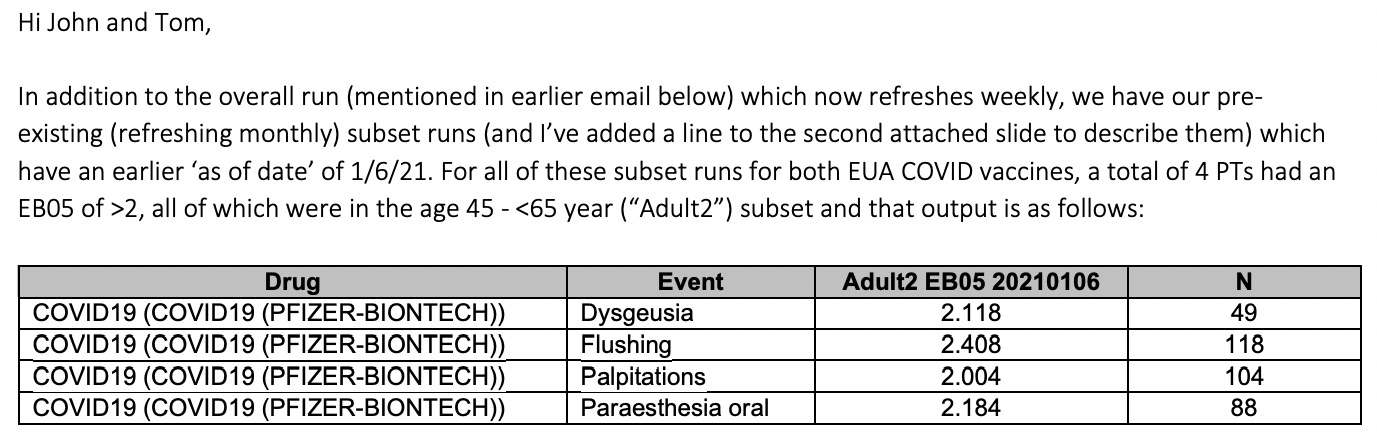
As of January 6, 2021, there were 4 Pfizer associated adverse event types with EB05s >2 reported.
But there’s one little number I would like to call attention to in this very long list of numbers that were included as part of disclosure to CDC employees in charge of COVID-19 injectable product safety signal assessments.
Go to page 99. Just one little line there. Under the heading: US Fatal EB05 20211210. I am assuming that this is indicative of safety signals associated with death with regard to vaccination failure as of December 10, 2021 since the heading US Fatal is not clearly defined in the document.
Vaccine-AE pairs ranked by lower 5% bound of EBGM confidence interval (EB05) Standard threshold for alert: EB05 ≥2 (page 2 from document)
The EB05 score provides a conservative estimate of the lower bound of the 95% confidence interval for the Empirical Bayes Geometric Mean (EBGM). This score is particularly useful in signal detection, such as identifying adverse drug reactions, where a high EB05 score suggests a significant association between a drug or drug combination and an adverse event. Typically, a large EB05 score (for example, over 1.5 or 2.0) is considered indicative of a potentially interesting interaction. (Brave search)


The EB05 is 2.731 in the context of fatality when the Meddra coded adverse event report was “Vaccination failure”.
THM: This was information passed in an email to CDC employees including Tom Shimabukuro and John Su in December 2021, and FDA employees. This information clearly - by their own assessment - indicates that this particular product (Janssen in this case) was ineffective in the context of people were dying.
Here’s one with the modRNA Pfizer-BioNTech product. The EB05 = 1.534 which is under 2 but over 1.5 under the “Fatal” heading, but over 2 in the general heading. You decide.

The EB05 is 1.534 in the context of fatality when the Meddra coded adverse event report was “Drug ineffective”.
And here are signals for Thrombosis and Pulmonary embolism in context of the Janssen product. Over 2 for general, at 1.784 and 1.513 for Fatal EB05.


I think this warranted reporting to a larger audience than internal chambers. I think that it’s a crime that it wasn’t. People had a right to know.
Here’s a good paper for additional reading.
More to come…

Addendum:
THM: VAERS data has been showing strong safety signals since January 2021 (see attached slide). Safety assessments were being done AND HIDDEN/NOT MADE TRANSPARENT with regard to proportional reporting ratio (PRR) and Bayesian (EB05) analyses of VAERS data from that time. Causality assessments should have been done, and the results made transparent to the public. They were not, and this effectively robbed the public of the right to informed consent. The products are now on the childhood vaccination schedule despite the fact that SARS-CoV-2 was never a threat to children. The COVID-19 products, as per the PRR calculations, clearly demonstrated association with serious adverse events in children ages 5-11 (see attached slide) as early as 5/20/2022, and this should have prompted immediate causality assessment, and cessation of use until definitive proof is provided to ensure no causal relationship.
Summary: David Menschik was reporting via email weekly to CDC officials Su and Shimabukuro (who you are probably very familiar with) the associations to various AEs using data mining and Bayesian analyses since January 2021.
Depending on whether you use an EB05 cut-off of 1.5 or a 2, the findings he reported would vary substantially since there are a lot of values between 1.5 and 2. he used a cut-off of 2, which is standard. The US Fatal EB05 score comprises the group of people who were reported to have died in the context of specific Meddra coded adverse events (AE) in the context of a specific COVID-19 product. What I wrote in my SS reminds us that Su and Shimabukuro did not report on the fact that the [Janssen] COVID-19 products were co-associated with death and COVID-19 at the time. At least, not that I ever saw.
The US Fatal EB05 score switched to value greater than 2 in October 8, 2021 to reach 2.128 in the context of "Vaccination failure", as pointed out in an email sent by David on October 12, 2021 to Su and Shimabukuro. The US Fatal EB05 score only increased from this date. NB: The Janssen shot AE "Vaccination failure" for which VAERS has many different versions of - from "COVID-19 breakthrough infection" to "Drug ineffective", had a US Fatal EB05 score higher than 2 for a long time. (my hypothesis is that this is one of ways that the signals can be dispersed to the point of being lost.)
October 2021, the US Centers for Disease Control and Prevention (CDC) began recommending it as a booster dose
October 2021, Janssen reported at a meeting of the US Food and Drug Administration Vaccines and Related Biological Products Advisory Committee (VRBPAC) that a single dose produced durable protection against severe disease and hospitalization for at least 6 months in the United States
February 2022, Johnson & Johnson announced it has temporarily suspended production of the vaccine
I don't know if Su and Shimabukuro just didn't notice or what, but nonetheless, they were being paid to notice and people were dying and the product continued to be recommended and was not suspended until 4 months later. Su and Shimabukuro - lead CDC employees - were the front men for the VAERS data (and other data) for passage of info to others as part of the Vaccines and Related Biological Products Advisory Committee Meetings.
eg: Shimabukuro - https://www.fda.gov/media/146269/download; https://www.fda.gov/media/159228/download (https://stacks.cdc.gov/gsearch?terms=Tom+Shimabukuro&collection=)
eg: Su - https://stacks.cdc.gov/view/cdc/110920 (https://stacks.cdc.gov/gsearch?terms=John+su&collection=)
The US Fatal EB05 score was greater than 2 as reported to Su and Shimabukuro (as per an October 12, 2021 email) for US Fatalities in the context of Janssen "Vaccination failure", indicating a definitive association between death and failure of the COVID-19 product. This should have prompted product removal and follow-up investigations into the efficacies of all COVID products.
The PRR data is old, but the thing about it is that PRR is the CDC's preliminary methodology (in addition to Bayesian analyses) to assess associated safety signals to prompt causality assessments. The PRR signals - if greater than 2 - should always lead to causality assessments. In many cases, the signals are not only greater than 2, they are off the scales. I would show the attached chart for 5-11 year olds (only SERIOUS reports). NB: This is comparing the COVID products to non-COVID products for specific AEs. In the case of COVID-19, the PRR is greater than 164. Don't forget to remind the Hearing members that for years, we were berated for even suggesting COVID-19 product associations with death, let alone causal effects. So many children were sacrificed and continue to be. There was never any need for the scandalous outcome: the COVID-19 shots on the childhood vaccine schedule, when SARS-CoV-2 was never a problem for children.
Cheers for sharing Jessica. Pretty conclusive, that EB05 metric...ought this be flagged to RFK Jnr as ammo to have the mRNA products withdrawn from market? Worth a direct contact to HHS now he's in office. I'm in Britland so we have the current moronic labour-run government, a total shambles here.
This is damning evidence. These are crimes. I hope this post goes far and wide….