
Mapping redundant or duplicate VAERS reports
Oh yeah, this is a thing. It's just not publicly available.

Aravind Mohanoor recently penned an article raising the idea that VAERS reports might get deleted for non-nefarious reasons. I think it’s possible, but more likely a mixture of nefarious and non-nefarious activities that lead to deleted reports.
I wrote the following on this subject matter in my paper “Critical Appraisal of VAERS Pharmacovigilance: Is the U.S. Vaccine Adverse Events Reporting System (VAERS) a Functioning Pharmacovigilance System?”:
Trained contractor staff are required to enter each VAERS report into the database, and if it should be deemed necessary to delete a VAERS ID from this database once entered, then it must be documented with a valid reason for the deletion. In addition, when a VAERS ID number is changed to a new number, this should also be documented by contractor staff.
It turns out, it likely is being documented and kept a big fat secret in a secret file labeled: big_stupid_secret_data.csv. Sorry, feeling a bit saucy.

Here’s some interesting stuff I found in the General Dynamics contract that I got ages ago by secret electronic stork delivery. This contract is an order for service from the CDC to General Dynamics Information Technology, Inc.,; the fifth largest defense contractor in the world by arms sales. By the way, you can go to article here at Jackanapes Junction to download the contract and read it for yourself.
BY ARMS SALES? Huh? I wrote this up before but I much like Polly the Parrot, I must reiterate in big letters: HUH?
Why was a defense contractor known for being successful in arms sales solicited by contract to sort out VAERS data in the context of SARS-CoV-related adverse event reports?
This should be the first and last question we ever need to ask on VAERS data analytic subject matter.
There are a few screenshots I am going to plop down here for everyone to peruse. I re-read the contract because word on the OpenVAERS street was that the contract stated that follow-up information with regard to VAERS IDs was to be kept hush hush and not publicized. Turns out, word on the street was true.
Go to the heading ‘TASK 3: VAERS FOLLOW-UP ACTIVITIES AND ENHANCED SURVEILLANCE’ (on page 16) as screenshotted here.

You’ll find point ‘F.’ on page 18 that includes details on how the follow-up data should be treated. It reads: “Follow-up information will NOT be included in the VAERS public data”.

Why not? Isn’t follow-up data vital information for the people who have submitted VAERS reports? Isn’t this information vital to the proper functioning of the VAERS system? Why is the follow-up only for the eyes of the ‘Government’?
Imagine this if you will. A person succumbs to myocarditis a few days after their second Pfizer shot. Said person submits a VAERS report online and receives a temporary VAERS ID. This person is contacted by vetters at CDC and verifies the details of the filing and in turn receives a permanent VAERS ID accessible in the VAERS public data available for download. I often call this ‘the front-end data’. Their VAERS report likely contains the MedDRA code ‘Myocariditis’ in one of their SYMPTOM fields. Now, imagine that a few weeks later, said person dies. Their GP attempts to update the person’s VAERS ID to indicate that the person succumbed to death. Here’s where it gets muddy.
How does this work? Does the GP call the CDC? Does the GP file the report using the online system? If so, does this ‘Secondary Report’ get merged with the ‘Primary Report’ based on variable field matches? Does this ‘Secondary Report’ get destroyed? According to the contract, the follow-up or updates never make it to the front-end data set.
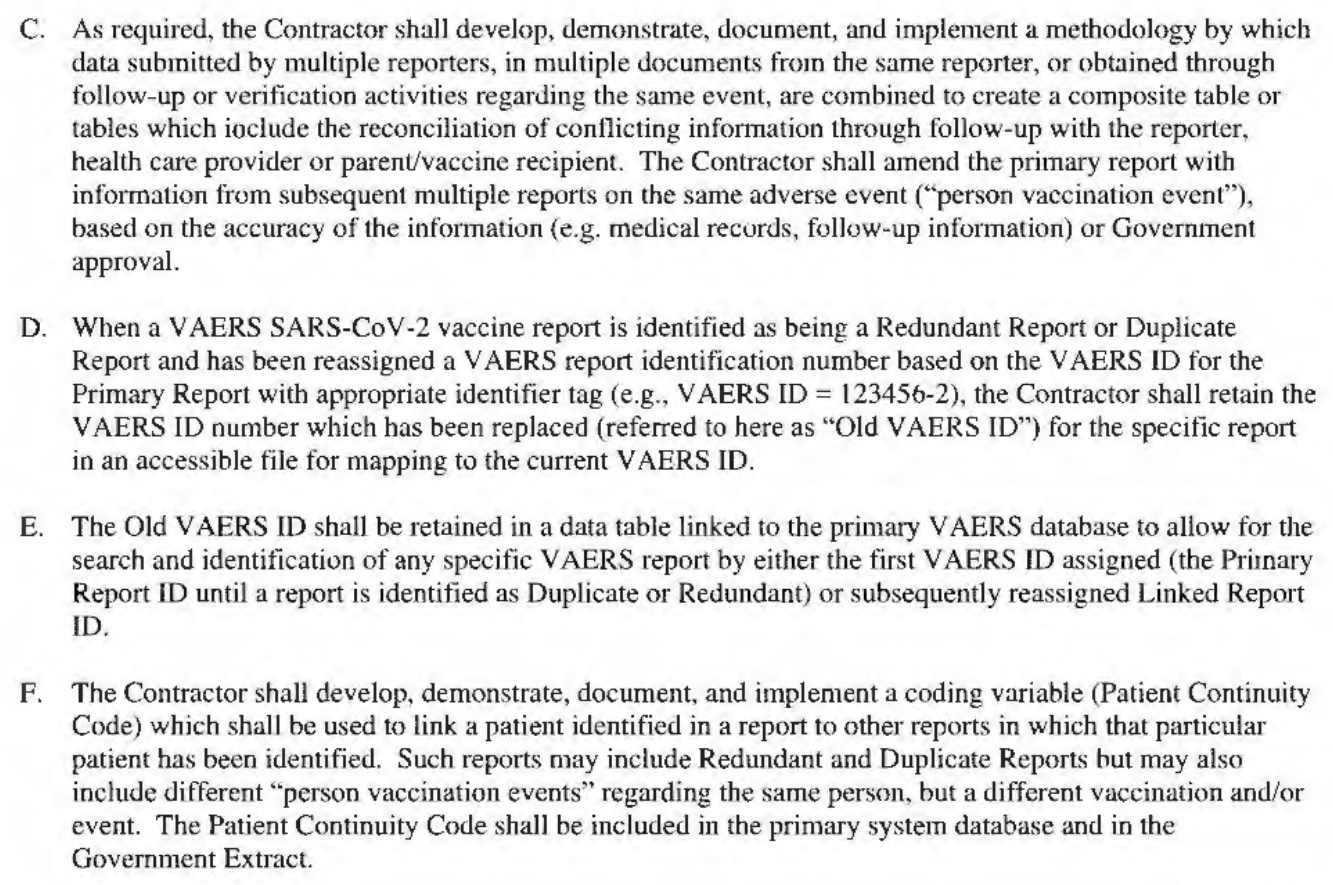
Read the following found on page 21 and 22 and see if you can figure out if such a death follow-up report would be deemed an ‘Exact Duplicate Report’ or a ‘Redundant Report’, or neither.


It seems to me, as it is written here, that if a person tried to update an existing VAERS report with a final diagnosis of death, they wouldn’t succeed. This is how I visualize it.
The GP would use the VAERS system and enter the same details into the system as before but this time enter ‘Death’ as the MedDRA code/adverse event. They may or may not be aware that the person had previously successfully filed a report. By my understanding of ‘d.’ as written above, the MedDRA code ‘Death’ would be ‘grouped together’ into the Primary Report which would have the original identifier VAERS ID attached to it. But what does ‘grouped together’ actually mean?
According to the next little tidbit in the following screenshot, ‘grouped together’ might mean that the follow-up data is indeed kept (ie: grouped together) but retained in a separate table (a narrative summary to the Government data - see screenshot below) that never makes it to the public data set. So in essence, all of the data and information exists, but us suckers will never see it.

Another disturbing possibility that OpenVAERS and others have contemplated is that the least severe adverse events of the bunch are selected to the front-end data, leaving behind the severe ones for ‘Government’ eyes only. It is possible that all of the ‘telling data’ is retained in the Government data set. We cannot know, but I suspect that as Liz put it, they are sitting on a goldmine of data and are doing this sitting knowingly. Can you spell FOIA?
Maybe that’s why they refer to the MedDRA codes as ‘Preferred Terms’: maybe they are ‘Preferred’ because they don’t reveal the true severity of the total list of adverse events? That was a joke, but also, not a joke.
Last point, they are tracking and mapping all of the data.
According to this contract, the contracted are in fact doing precisely what I had suggested in my paper: they are retaining ‘duplicates’ and additional data in accessible files for mapping to current VAERS IDs. The problem is, the public is not entitled to this information. This is a very slippery slope. If the public is not able to verify the validity of an omitted report, then how can we know it was valid to omit a report?
I reiterate:
VAERS is designed to reveal potential early-warning risk signals from data, but if these signals are not detectable as they are received, then they are not useful as warnings. Considering the relevance of safety concerns in the face of the large numbers of AEs being reported into the VAERS system in the context of COVID-19 products, it is essential that the VAERS system be carefully and meticulously maintained. Despite the emergence of the Standard Operating Procedures (SOP) for COVID-19, VAERS is lacking in transparency and efficiency as a PV system, and it requires amendment or replacement.
And furthermore:
The deleted data from the total VAERS ID count are individuals enrolled in post-market surveillance human-subject studies: the where- abouts of their VAERS reports of death need to be accounted for. There is absolutely no reason for these data to be missing, from what can be ascertained. If the data were false, as was suggested as the only reason to delete an entry, then there needs to be a record of this edited data made available with the publicly available VAERS data.
I rest my case. Again.
Please, go on and hang in there.... we are all with you Jessica!
My sense is that somewhere in the bowels of these systems the government with the help of AI no doubt to make it faster is assiduously tracking every little bit of data that they can while simultaneously pretending to be as dumb as possible about it. The likely reason is to hide the true extent of the crime against humanity while having all the receipts, just as the Nazis did. Of course there would be front end loading of symptoms: someone who used the system in the first few days after the jabs but who never recovered and eventually died would not have that data tracked by the people the system was set up to alert. People would want to know if that person with myocarditis recovered or died, or that person with seizures got better or didn't. There can be no trust without transparency