


In case you thought getting more shots was a good idea...
It's really not. Show your folks.

A new preprint is out entitled: “Risk of Coronavirus Disease 2019 (COVID-19) among Those Up-to-Date and Not Up-to-Date on COVID-19 Vaccination”1 and it concludes from a multivariate analysis of 48,344 individuals (Employees of Cleveland Clinic) that ‘those not “up-to-date” on COVID-19 vaccination had a lower risk of COVID-19 than those “up-to-date”’.
I can already hear the hit piece vultures circling and chanting: it’s not peer-reviewed. No it’s not, but read it anyway and ask yourself if this study has merit. Decide for yourself. Maybe my summary can help.
What did they do?
They looked at the differences between ‘infection rates’ (cumulative incidence) with COVID-19 in individuals who’d received the bivalent shots treating injection with the COVID-19 bivalent product as a time-dependent covariate. What this means is that they accounted for the fact that injection status can change per individual at any time (injection time), and at each injection (event) time, that current status of the individual is compared with the current values of all others who were at risk of COVID-19 at that time.
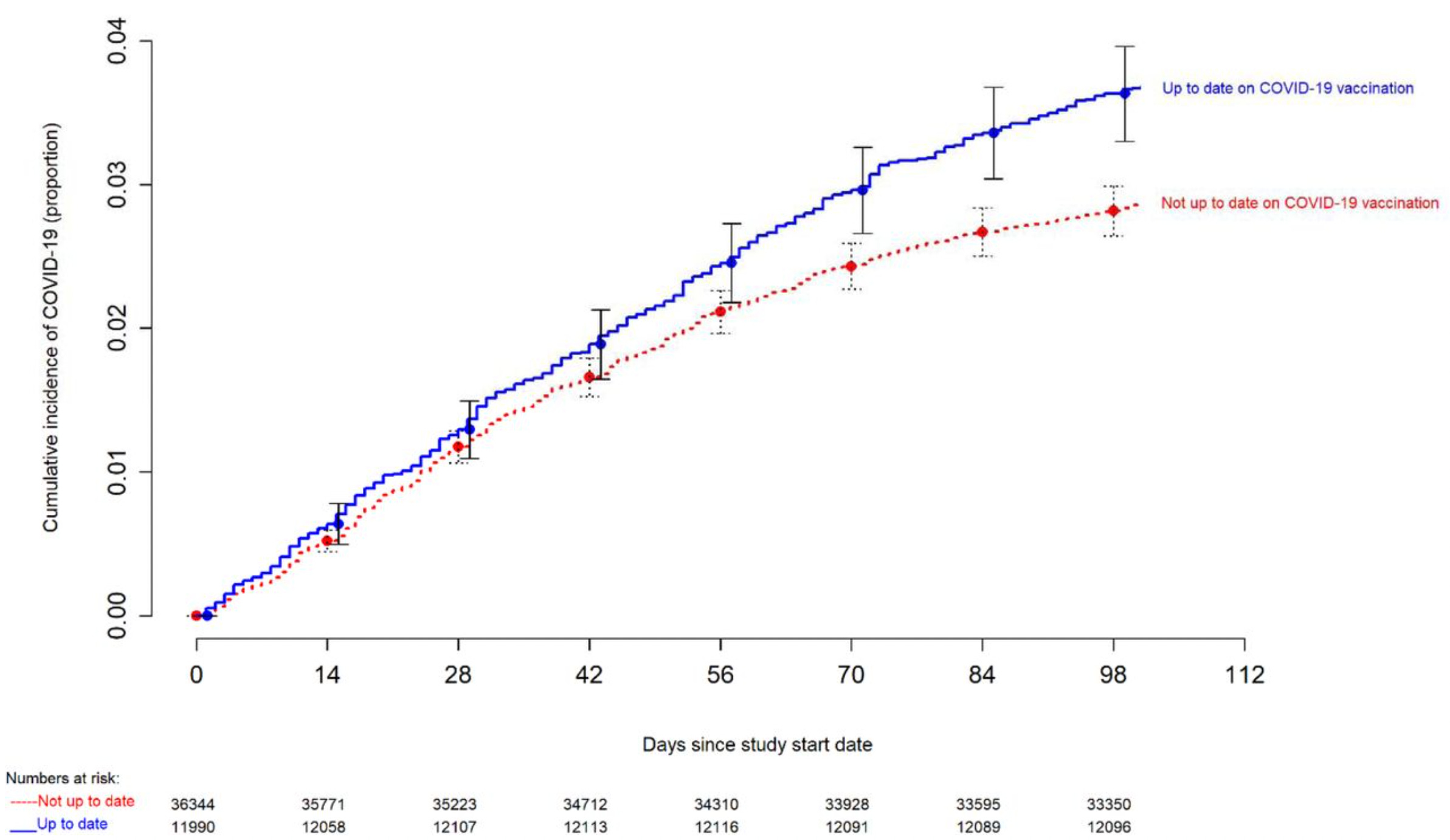
So they collected and compared two rates: incidence rate for ‘up-to-date’ and ‘not-up-to-date’ which were calculated by dividing the number of individuals in each group who reached the outcome - COVID-19 (as determined by ‘testing’) - by the number of individuals either injected or not.
It is very clear from Figure 1 in the preprint that the risk of getting COVID-19 is lower if you are not up-to-date (red). As time progressed (from the end of January 2023), the disparity between the two groups becomes more apparent. Who here is surprised?
Covariates collected were age, sex, job location, and prior SARS-CoV-2 infection. Since the propensity to get ‘tested’ for COVID-19 can vary among individuals, here it was defined as the number of COVID-19 nucleic acid amplification tests (NAATs) done divided by the number of years of employment at Cleveland Clinic Health System (CCHS) during the pandemic.
When they stratified propensity to get tested, for each tertile, they observed that the COVID incidence was higher in the ‘up-to-date’ group even when the propensity to get tested was low (green).

They also used multivariable Cox proportional hazards regression - which is a survival model that relates the time that passes, before some event occurs, to one or more covariates that may be associated with that quantity of time2 - to determine any potential association of various variables with time to COVID-19 (the outcome).
According to the model, adjusted for COVID-19 test propensity, age, sex, and phase of most recent SARS-CoV-2 infection, “not-up-to-date” status was associated with a lower risk of COVID-19 (HR, 0.77; 95% C.I., 0.69-0.86; P-value, <0.001) as shown in the blurry table below. The covariates minimally effected the the adjusted Hazard Ratio (HR) as seen when comparing the Unadjusted HR and Adjusted HR columns.

Ultimately, the authors found that the prior ‘infection’ (and robust immunity acquired from said infection), was deterministic of future COVID-19 status, ie: lower risk for COVID-19.
Infection is superior to injection with regard to COVID-19 repeat infections.
Therefore it is not surprising that not being “up-to-date” according to the CDC definition was associated with a higher risk of prior BA.4/BA.5 or BQ lineage infection, and therefore a lower risk of COVID-19, than being “up-to-date”, while the XBB lineages were dominant.
And finally, the authors write:
It is now well-known that SARS-CoV-2 infection provides more robust protection than vaccination.345
Yes, it is well-known. It was well-known before. Vaccination can ever only hope to be second best to natural immunity, in my opinion.
Best vaccination scenarios can prevent severe symptom onset where the injection material is not more harmful than helpful in generating targeted immune responses for challenge situations.
Worst vaccination scenarios can cause more harm than good, as is seemingly being demonstrated with the gene-based therapies introduced to the human population at the beginning of the COVID era.
When the medicine is more harmful, ie: associated with higher morbidity, than the disease, then it is time to stop calling it medicine.
Nabin K. Shrestha, Patrick C. Burke, Amy S. Nowacki, Steven M. Gordon. Risk of Coronavirus Disease 2019 (COVID-19) among Those Up-to-Date and Not Up-to-Date on COVID-19 Vaccination. medRxiv 2023.06.09.23290893; doi: https://doi.org/10.1101/2023.06.09.23290893.
https://en.wikipedia.org/wiki/Proportional_hazards_model
Shrestha NK, Burke PC, Nowacki AS, Terpeluk P, Gordon SM. Necessity of Coronavirus Disease 2019 (COVID-19) Vaccination in Persons Who Have Already Had COVID-19. Clin Infect Dis Off Publ Infect Dis Soc Am 2022; 75:e662–e671.
Gazit S, Shlezinger R, Perez G, et al. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. 2021: 2021.08.24.21262415.
León TM, Dorabawila V, Nelson L, et al. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May– November 2021. MMWR Morb Mortal Wkly Rep 2022; 71:125–131.
Thank you again....I cannot thank you enough for doing this critical sharing with us...already sent it to my Mom....I keep trying, but she never wants to discuss anything related to the jabs.....what more can I do? As Desmet said, we have to keep trying, and use our voices. It would seem just so wrong to do otherwise.
My daughter-in-law and 2 adult grandkids all had 4 shots so far. They take pcr tests when they have sniffles. They won’t listen to anyone about not taking more shots. Her parents are the same. It’s the weirdest thing I’ve ever seen.