


Debunking the yellow dot lot placebo theory...
What do the VAERS reports look like for the yellow (and blue) lots in the Schmeling, Manniche, Riis Hansen study?

There’s been a suggestion in the media based on the work by Max Schmeling, Vibeke Manniche and Peter Riis Hansen entitled: “Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine” published in the European Journal of Clinical Investigation, that the batches associated with very few or no adverse events are in fact, placebos.
I recommend watching this video for background.
Below is the graph from the Schmeling et al. study that shows 3 distinctly different groups of vax lots brought to you by Pfizer (BNT162b2). They examined adverse event data administered in Denmark (population 5.8 million) from December 27, 2020 to January 11, 2022. The difference between the 3 groups is defined by the number of adverse events associated with each lot. Each lot has a different number of doses and for the purposes of this analysis, all of the doses in each batch were administered to the Danish people.1
N.B. SAE = ‘Suspected adverse events’ in the Schmeling study whereas SAE = ‘Severe’ or ‘Serious’ adverse events as per the convention with respect to VAERS. So when I write ‘SAE’ I mean a Serious Adverse Event (ie: death, hospitalization, emergency room visit, birth defect, life threatening or disability).2
P.S. ADRs = adverse reactions = adverse events = AEs

The yellow dots all lie on or very near the x-axis meaning they are not (or minimally-) associated with adverse events. There are 18 of them. I decided to embark on an analysis in an attempt to answer the question:
Are the yellow dot lots placebos?
I do not think we can say this. In fact, as my analysis shows, there are many SAEs associated with the yellow dot lots and with a more comprehensive data set, it is easy to see that the yellow dot lots are far from placebos.
Denis Rancourt points out that the lack of information pertaining to the subjects could provide a recipe for seeing artifacts that may arise due to differences in who was injected with what when. Did you like that? And I agree. For example, the elderly were picked on first, have a higher inherent proclivity for death, and received different batches than the later roll-out victims. Perhaps this could explain the blue dots?
The yellow dot lots are the following: FG9019, FH3219, FH8469, FJ3438, FJ4187, FH3220, FM3092, FL1072, FN3731, FK9706, FM3802, FK0115, FN3758, FK8911, FK9412, FM3289, FM9088, FN5519. One of these vax lots (emboldened) is associated with 5 deaths according to the original data passed to me by Max Schmeling (thank you). By the way, the authors of this work are very transparent and interested in real science, in my opinion.
On the Danish data
1.1 The yellow dots
Only 4 (12%) of the yellow dot lots - proposed to be ‘placebos’ by some - were not associated with AEs. In the case of 5 (28%) of the yellow dot clot shot lots, 100% of the AEs comprised SAEs. Half of the yellow dot lots have AEs that are considered SAEs more than half of the time.
Here are some observations of the raw Danish data that make me skeptical about the ‘placebo’ theory of the yellow dot clot lots, in spite of the fact that the absolute number of AEs is low (relative to the blue dot lots):
A low percentage of lots are not associated with AEs (12%)
61% of the lots are associated with SAEs
One of the lots is associated with 5 deaths (7% rate in AE reports and 16% rate in SAE reports)

On VAERS data
I queried the VAERS data within the December 27, 2020 to January 11, 2022 timeframe, and all for all existing reports (December 27, 2020 to June 30, 2023): I wanted to see how many more reports for these lots have been filed since the beginning of 2022. It is possible that what was showing up in the data, is currently not, or vice versa. Bigger sample sizes are always better as statistical power can increase.
It is important to note that I do not have the ‘Doses’ (dose number) for the relevant yellow vax lots as per the VAERS data. It is a pity. If I had this data, I could provide a much better analysis. For the purposes of this analysis, I assume that the batch sizes per lot are equal. This might be a very bad assumption, but what can I do?3 I’m still better than the CDC staff, combined.
2.1 The yellow dots in the timeframe-matched VAERS data
Of the total lots, 6 (33%) are not associated with AEs (Table 2). Wow! That’s even better than the Danish data. This is the first indication that these lots might be considered to be placebos, especially since 3 of these (FK9412, FM9088 and FN5519) match the Danish AE data.

2.2 The yellow dots in the extended VAERS data
The first notable difference (Table 3) is that 100% of the lots are associated with AEs, and SAEs. If all of these lots are associated with SAEs - and in some cases hundreds - then they would never classify as placebos in my books. One might argue that since the absolute counts are relatively low (when compared to the blue dots), that the yellow lot group members are still contenders for the classification of ‘placebo’ with regard to AE association, but I would argue against that argument. They don’t know that we know that they know that we know.
Nowhere in my thinking, even if half a million shots were administered, is 377 SAEs placebo-qualifying. That’s very nearly 1 SAE (potentially deaths) per 1,000 shots.

The most important distinction between the restricted timeframe and the extended data sets is that when the data is more populated (more complete), there are no longer lots that are not associated with AEs. In addition, the more complete data set tells us that for every one of the yellow dot lots, there were SAEs reported.
Interjection
It is my opinion that we have still only seen the tip of the iceberg with regard to the harms imposed by these modified mRNA COVID injections. For the younger individuals, who started off strong and healthy, it will be a longer road to pathology and it is quite likely that a very small proportion of these individuals will even report their condition to VAERS because let’s face it, who’s going to associate a cancer they ‘get’ a year or two out from their latest Pfizer shot? Nonetheless, VAERS will continue to be fed.
It is worth noting here, that often times SAEs don’t get classified as they should be when entered into VAERS. For example, someone can experience severe chest pain complete with a myocarditis diagnosis but with no report of a hospital visit in VAERS. So again, these numbers are underestimates and this data is highly under-reported. And on the subject of potential biases, reporting biases are surely contributing to differences in AE and SAE counts in disparate data sets.
At this point, my brain is getting closer to being convinced that these lots are not placebos.
Comparing the Danish and VAERS data (timeframe-matched and extended) using boxplots
Perhaps a more visual demonstration is required. Below is a boxplot showing the medians and distributions of the yellow dot lots for the Danish and VAERS timeframe-matched data (left) and expanded data (right).

Boxplots are nice because they give an easy to interpret visual of how the data is spread out about the medians (the middle values in the data sets). The dots are the outliers - meaning that they are kind of in a league of their own. The lines or ‘whiskers’ (meow) indicate the variability outside the upper and lower quartiles (the medians of the top higher- and lower-valued chunks of data within the groups).
On the left, there’s no real difference, is there? In fact, there is no statistical difference (Mann-Whitney U test → p-value is 0.56868). The variability is higher in the VAERS timeframe-matched data (yes, the data sets are tiny so 3 outliers matter), but the medians are the same. This variability becomes more pronounced with the expanded VAERS data set as shown on the right. The medians are quite different and in fact, this difference is significant (Mann-Whitney U test → p-value < 0.00001). These results are mimicked for the SAE expanded and timeframe-matched VAERS data (p-value < 0.00001; p-value = 0.78716, respectively.)
This means that with a more comprehensive data set, the ‘placebo-ness’ of the yellow dot lots is lost. If we plot the (S)AEs according to the original data and the VAERS extended data (Figure 3), 2 things are clear:
The blue lot and the yellow lot groups are disparate, regardless of the data source (statistically significant Danish: p-value < 0.00001; VAERS: p-value < 0.00001).
The yellow lots are not placebos.
The blue dot lots are likely the batches administered early in the roll-out to our elders - who do have a higher proclivity for death than the younger folks who were injected later - I would bet that the blue dots are the old who died first having been injected with batches administered early-on in the roll out.

As can be demonstrated from Figure 3, in the case of the VAERS extended data, there are very nearly 1/1,000 SAEs reported for lot FH8469 and therefore, I think we can all agree, that does not a placebo make.
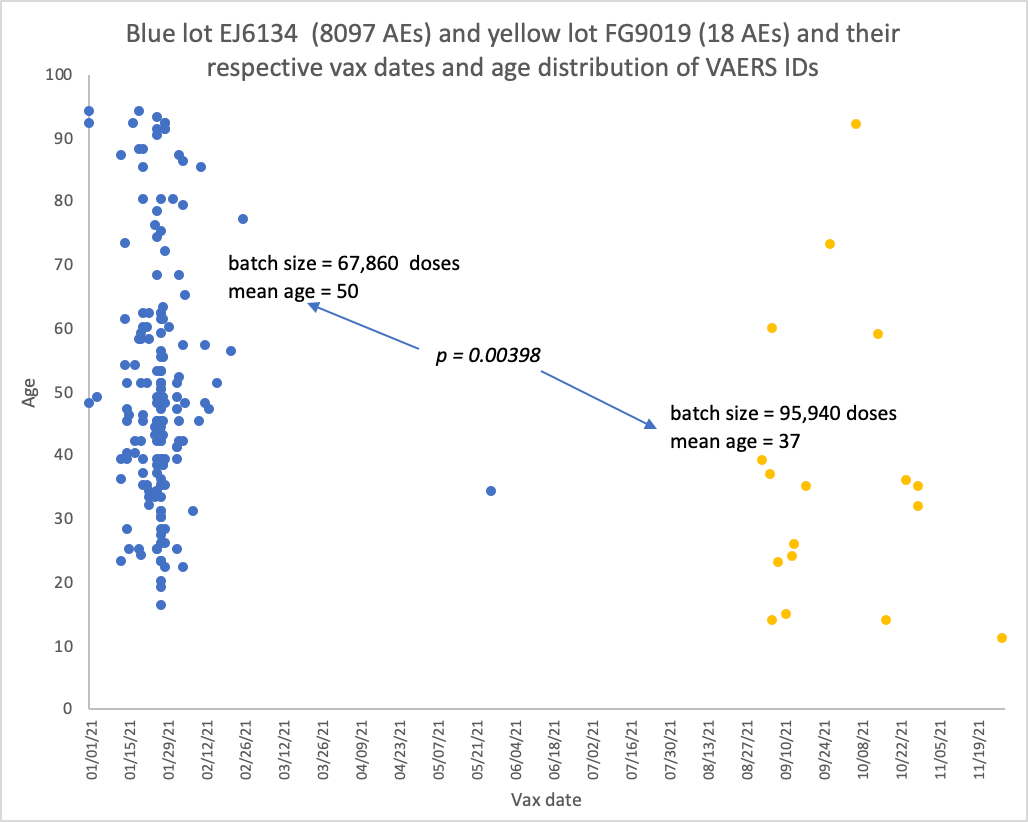
One last thing. There is a way to check the hypothesis “the blue dots are the old who died first having been injected with batches administered early-on in the roll out”. VAERS is amazing because it has 52 different variables to choose from. One of them is the vax date. Sure, it would be wicked if I had manufacturing date data for these lots but I don’t, so the vax date data is a good proxy. I checked the vax dates - and the ages - for the SAEs associated with the blue and yellow dots. As shown in Figure 4, I checked the ‘worst’ blue lot EJ6134 and a randomly-selected yellow lot FG9019.
There is a statistically significant difference in the ages between the blue and yellow lots (p-value = 0.00052). The mean age for the blue dot lot SAEs (9 of them) is 58 years of age, and for the yellow dots (10 of them), 43. What is crystal clear in the example in Figure 4, are the differences in vax dates between the blue and the yellow lots. It doesn’t happen very much in data science that something so clear cut comes out of a query. The reports filed for EJ6134 were pretty much all injected in January and February of 2021 and the reports filed for FG9019 were pretty much all injected in September-November of 2021.
So, it appears as though a good explanation for the distribution patterns seen in the Danish study is due to batches administered earlier to older individuals. To be perfectly fair though, there must be variability between batches and even doses based on manufacturing and handling of these products.
Conclusions
The blue lot and the yellow lot groups are disparate, regardless of the data source (statistically significant Danish: p-value < 0.00001; VAERS: p-value < 0.00001)
The yellow lots are not placebos.
The blue lots appear more deadly likely because of who they were put into - the elderly.
The yellow dots appear innocuous because of a limited data set and likely because of who they were put into - the younger folks.
Ok. I think that’s it for now. Please do comment.
By the way, this analysis in no way minimizes or undermines the findings in the Schmeling et al. study. They are absolutely right-on about those groupings, at least in the context of the blue and yellow groups. Hashtag: thegroupingsarereal.
It does, however, debunk the ‘yellow dot lots are placebos’ theory.
“Thank you for all your work and thank you very much for your thoughts on our study. I just wanted to add, that the lot size data, we obtained from The Danish Serum Institute, is in fact the number of doses pr. batch, that were shipped from the Danish Serum Institute to all the Danish vaccination centers. It is perhaps the data, that comes closest to being the real number of administered doses pr. batch, since the shipped doses exclude any doses, the Serum Institute might have in stock.
I should also mention that the ADR data, is in fact collected much the same way as VAERS, but the quality is in my opinion much better. Of all the known reported batch numbers only, a mere fraction does not validate correctly towards the lot size list.
I'm guessing this is one of the unexpected and unintended beneficial side effects of living in one of the countries in the world that collects and registers the most data about their citizenry.” Max Schmeling
https://vaers.hhs.gov/docs/VAERSDataUseGuide_November2020.pdf
It is also notable that the VAERS data includes reports filed from all over the world, but according to the SPLTTYPE variable (that tells us where the report was made), none originated from Denmark. There were only a few with information that indicate reports filed from Brazil, Montenegro, New Zealand, South Africa, Japan, Switzerland, United States, Moldova and Australia. (This is in reference to the front-end database of VAERS.)
I think it was Ryan Cole who postulated that some of the less harmful batches may be due to defective manufacture, such that they are almost inert, but not quite placebo as you say. And Sasha Latypova pointed out how complex the manufacturing process is, and how difficult it would have been to ensure any kind of quality control, especially given the scale and speed of production.
Do we have any idea where the different batches were made?
Jessica, nice analysis. I sent you the number of doses data for Denmark. The number of doses was not equal between the lots, far from it. There are 2 issues. The lots in EU were split and distributed to different countries in unequal numbers of doses per each lot number. They did the same in the US across different states. The second issue is that as in the US, the "toxicity" of lots for THE SAME lot number looks very different depending on the location (country/state). The only explanation I can come up with - they are fraudulently marked as "the same" lot but produced on different production lines, possibly active ingredients coming from different locations. That's why same lot looks very different depending on the country/US state. In fact in the US, in the shipment data that Aaron Siri FOIAed it is clear that toward later time period "one lot" of product is not one production run. Today Pfizer has switched to "continuous manufacturing" so lot numbers are meaningless. This can also be the difference between the "early" and "late" lots - early were the single production runs and later ones are a mixture of many production runs from multiple locations/lines. It's not the age of the recipient. Even if there is a difference in the median - the vertical dispersion of the batches that you see on your graph - that's gigantic and not explained by age.